


















 63 / 66
63 / 66

CARDIOVASCULAR JOURNAL OF AFRICA • Volume 32, No 3, May/June 2021
AFRICA
173
discharged, he took no beta-blockers or angiotensin converting
enzyme inhibitors (ACEIs). His BP was in the normal range and
activity tolerance returned to normal levels. TTS did not recur
after the tumour was removed during follow up of a year.
Discussion
Pheochromocytomas are uncommon catecholamine-secreting
tumours. Intractable hypertension is one of the most common
symptoms, accompanied by headache, palpitations and
perspiration. Pheochromocytoma crisis, with an occurrence rate
of about 10%, induced by sudden release of large amounts of
catecholamines, is a dreaded and potentially lethal complication
of pheochromocytoma. Clinical manifestation consists of severe
hyper- and/or hypotension, high fever, encephalopathy and
multiple organ system failure.
5
Haemodynamic abnormality of pheochromocytoma crisis
has a variety of causes such as cardiomyopathy, myocardial
infarction, arrhythmia, pulmonary oedema, cerebrovascular
accident, encephalopathy, liver and kidney failure, adrenal
haemorrhage and others. Spontaneous rupture of adrenal
pheochromocytoma, one cause of pheochromocytoma crisis,
is rare, and most of such rare cases present as haemorrhagic
shock.
4
Here we discuss a case of a young man with adrenal
pheochromocytoma rupture developing pheochromocytoma
crisis, which presented with basal TTS and cardiogenic shock.
Pheochromocytoma serves as a distinct physical trigger
of TTS, and TTS may be found in up to 3% of patients
with pheochromocytoma and paraganglioma.
3
The types of
pheochromocytoma-induced TTS (pheo-TTS) differ significantly
in all patients with TTS (all-TTS), with the basal type in almost
30% of pheo-TTS and the global type in 20% of pheo-TTS. Both
types are rare in all-TTS, with the basal type only accounting
for 2.2% of all-TTS and the global type even less. Patients
with pheo-TTS are significantly younger than all-TTS, with
a relatively high proportion of men. In addition, pheo-TTS
is characterised by a dramatic clinical presentation with high
complication rates, especially in patients under 50 years, and a
relatively high recurrence rate.
Common complications are heart failure (occurrence rate
51%), pulmonary oedema (45%) and cardiogenic shock (34.6%),
which occurs more frequently in the global and basal patterns
of pheo-TTS than the apical type.
6
As reported in most previous
cases, levels of cardiac biomarkers are slightly or moderately
elevated,
7
but were significantly increased in our patient.
In this case, thepatient presentedas acutemyocardial infarction
initially, with ECG changes presenting as ST-segment elevation
and depression, cardiac biomarkers significantly elevated, and
wall-motion abnormality of the LV on TTE. However, this
young man had no chest pain, no history of hypertension,
diabetes mellitus, smoking, or family history of early-onset
coronary heart disease. TTE showed akinesis/hypokinesis of the
entire basal and middle LV segments, which extended beyond
a single epicardial vascular distribution. These features and
the presence of physical stress of pheochromocytoma rupture
pointed to the basal type of TTS. Regular TTE showed LV wall
motion distinctly improved on the 12th day and almost recovered
after 17 days, which indicated LV dysfunction was transient and
confirmed the diagnosis of TTS.
A coronary CT angiogram should be performed to exclude
coronary artery diseases, but at that critical time, with life support
of IABP and ventilator, the patient had no chance of getting
a CT angiogram. In this patient, severely impaired LV systolic
function with an EF of 27% caused by TTS was one of the main
causes of shock. His haemoglobin and red blood cell count were
in the normal range, so haemorrhagic shock was excluded.
The precise pathophysiological mechanisms of TTS are
incompletely understood, but there is considerable evidence that
catecholamine excess and sympathetic stimulation is central
to its pathogenesis.
8,9
Catecholamine levels of this patient were
significantly elevated. We supposed that the sudden release
of large amounts of catecholamines from the ruptured
pheochromocytoma played an important role in the pathogenesis
of TTS in this patient. However, the reason why the basal type of
TTS has a high incidence in pheo-TTS remains unclear.
Alhough reports of pheochromocytoma causing TTS are
not uncommon, spontaneous rupture of pheochromocytoma
causing TTS is extremely rare because of the low incidence of
tumour rupture. So far, only one case diagnosed with apical TTS
caused by pheochromocytoma rupture has been reported around
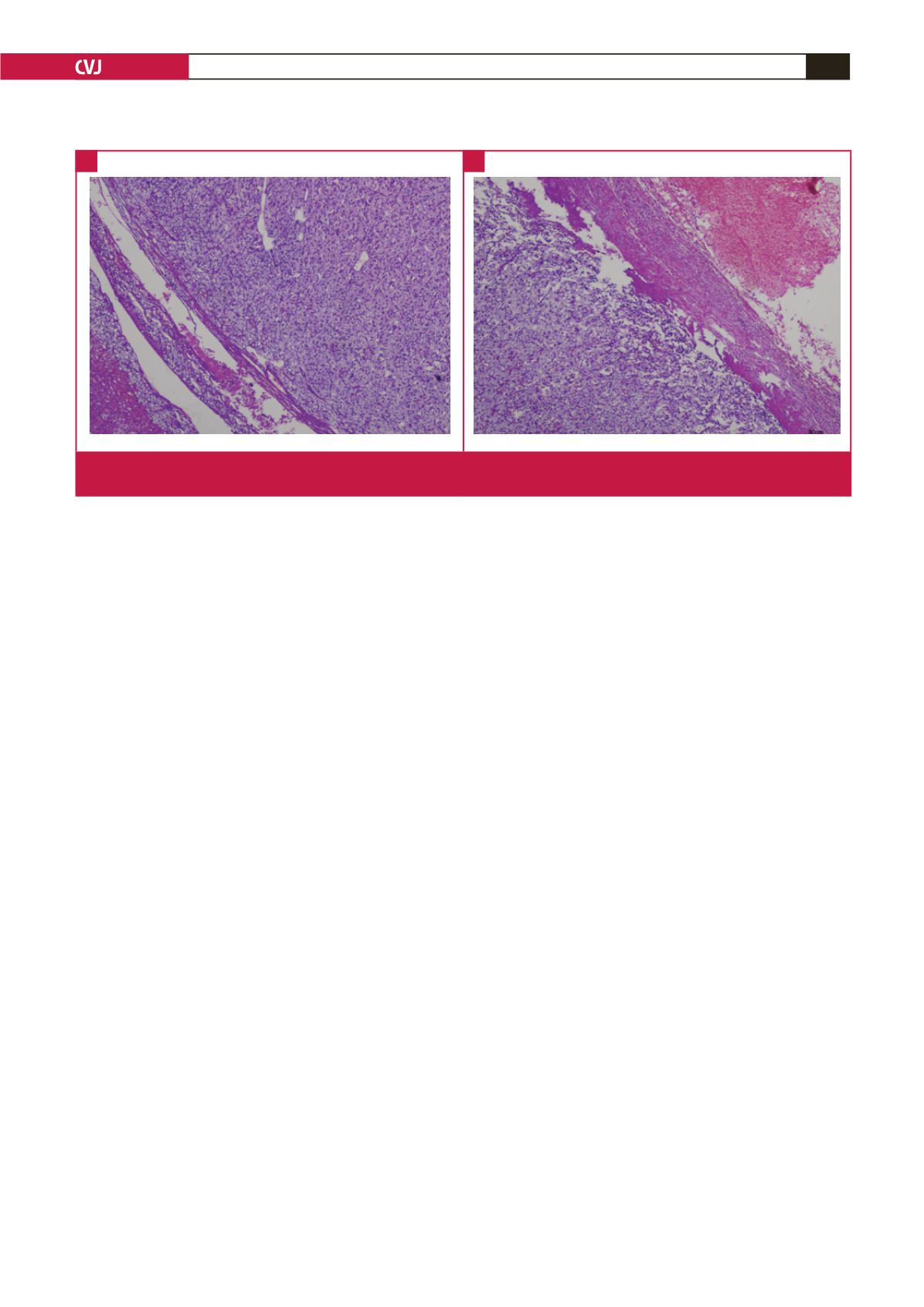
Fig. 3.
A. The pathology examination revealed an adrenal pheochromocytoma. B. Haemorrhage and rupture of the pheochromo-
cytoma.
A
B