


















 7 / 66
7 / 66

CARDIOVASCULAR JOURNAL OF AFRICA • Volume 32, No 3, May/June 2021
AFRICA
117
revealed that LAA morphology has a close relationship with
stroke.
The LAA is the main site for thrombosis in NVAF patients, and
LAA morphology affects the incidence of stroke. In this study, we
sought to determine whether LAA morphology could predict the
formation of LA/LAA thrombus in patients with NVAF.
Methods
This study was a retrospective review of transoesophageal
echocardiography (TEE) and electronic clinical records.
9
The
ethics committee of Changhai Hospital approved the study
protocol and written informed consent was obtained from all
patients before enrollment.
We searched the TEE databases of Changhai Hospital
for patients undergoing consecutive TEE imaging between
2010 and 2016 while in drug-refractory NVAF undergoing
catheter ablation or cardioversion. Excluded NVAF patients
were those taking warfarin with an international normalised
ratio (INR) ≥ 1.5, subjects injecting low-molecular weight
heparin subcutaneously, taking heparin intravenously or taking
new anticoagulants, and those with chronic kidney disease,
malignant tumour, connective tissue disease, valvular heart
disease or hyperthyroidism. Patients were also excluded if they
had rheumatic valve disease or a history of mitral valve repair
or mechanical valve implantation. Finally, 555 patients were
selected for analysis in this study.
All NVAF patients were divided into two groups, a thrombus
and a non-thrombus group, according to TEE. The thrombus
group had a thrombus or a change of ‘mud’ in the LA/LAA, and
the non-thrombus group had no changes in the LA/LAA.
LAA imaging was obtained using 320-channel cardiac CT
angiography (Toshiba Aquilion ONE) with volume-rendering
post-processing technology (using the Vitrea Enterprise Suite)
to reconstruct its three-dimensional structure. The atria were
divided into chicken wing, cauliflower, cactus and windsock
types
10
by two experienced cardiac CT radiologists blinded
to the other clinical data. Each morphological classification
represented a consensus decision by both radiologists. No
statistically significant bias was detected in the classification of
the LAA by the radiologists.
The CHADS
2
and CHA
2
DS
2
-VASc scores were calculated for
each patient. The CHADS
2
score includes risk factors for the
presence of congestive heart failure, hypertension, diabetes, age
≥ 75 years, stroke or TIA. In addition to stroke or TIA (which
confers two points), the presence of the other risk factors adds
one point to this score. The CHA
2
DS
2
-VASc score is modified by
the addition of further risk factors for stroke such as vascular
disease, age 65–74 years and being female.
11
In order to compare the ability of the two scoring systems
(CHADS
2
and CHA
2
DS
2
-VASc) to predict LA/LAA thrombus,
we graded and grouped all patients with the three scoring
systems. A score of zero, one and two points or more were
utilised to define low-, intermediate- and high-risk groups,
respectively, and we then compared the intermediate group score
to that of the other groups.
12
Renal dysfunction was defined as a low estimated glomerular
filtration rate (eGFR) < 60 ml/min/1.73 m
2
. The eGFR is
calculated using the abbreviated Modification of Diet in Renal
Disease Study equation:
eGFR (ml/min/1.73 m
2
) = 186.3 × [serum creatinine (mg/dl)]
-1.154
× age (years)
-0.203
(or if female × 0.742).
13
TEE is currently the gold standard for diagnosis of LA/LAA
thrombosis.
14
Before a LA/LAA thrombosis develops, the blood in
the LA/LAA manifests two dynamic changes, ‘smoke’ and ‘mud’.
During the smoke phase, spontaneous ultrasound imaging of the
LA reveals dynamic swirling (or smoke-like) echo signals when
imaged at optimal gain settings.
15
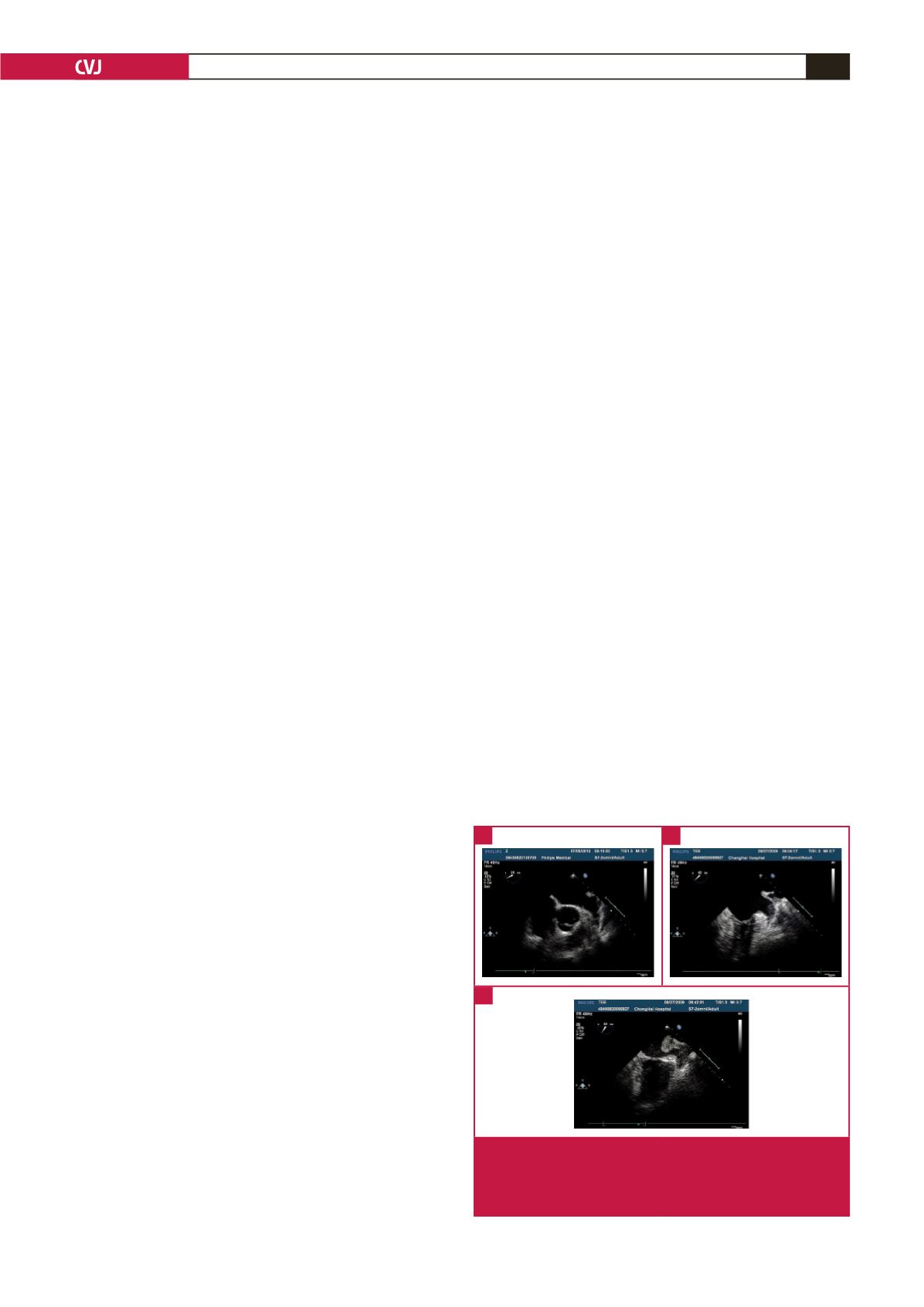
Mud signals (Fig. 1A) on TEE
reveal a mass structure that is relatively clear with a gelatinous
appearance.
16
Thromboembolism (Fig. 1B) is visualised through
multiple angles as a discrete mass from multiple windows and the
mass is independent of the endocardium and pectinate muscles.
17
Generally TEE can identify a thrombosis larger than 2 mm. In
our study we categorised mud and thrombosis images as LA/
LAA thrombus-positive. Images without LA/LAA mud or
thrombus were classified as negative for clots (Fig. 1C).
LAA morphology was classified on the basis of the number
of bends in the lobes, the location of origin from the LA and
the number of lobes.
18
The radiologists who interpreted the CT
images were blinded to the history of the patients, to minimise
the risk of bias.
Chicken wing LAA consists of a main lobe and has an
obvious bend in the middle or on the base of the main lobe, or
the LAA main lobe has an anatomical fold towards the direction
of the LAA openings. This LAA morphology usually has
secondary lobes or twigs.
In the cauliflower LAA there is usually no main lobe, but there
are secondary lobes of varied number among individuals and
with limited length. This LAA morphology usually has a complex
internal structure. Because of the large variability in morphology,
the LAA ostia have less regularity and could be oval or round.
The cactus LAA morphology mainly has a dominant central
lobe with secondary lobes extending in both superior and
inferior directions. The windsock LAA has a long main lobe with
a variety of possible morphologies related to the location and
number of secondary or even tertiary lobes (Fig. 2).
10
Fig. 1.
Spontaneous ultrasound imaging of different changes
of blood in the LA/LAA. A: with mud variation in the
LAA, B: with thrombus variation in the LAA, C: without
mud or thrombus variation in the LAA.
A
C
B