


















 10 / 66
10 / 66

CARDIOVASCULAR JOURNAL OF AFRICA • Volume 32, No 3, May/June 2021
120
AFRICA
Discussion
To the best of our knowledge, this is the first study to incorporate
LAA morphology into a modified CHADS
2
score, leading to
the L
2
CHADS
2
risk score (L with two points). We compared
the predictive accuracy of the CHADS
2
, CHA
2
DS
2
-VASc and
L
2
CHADS
2
scores in predicting thromboembolic events in
patients with NVAF. The main findings were as follows: (1)
LAA morphology was closely related to LA/LAA thrombus; (2)
the L
2
CHADS
2
score could reliably predict LA/LAA thrombi,
and the L
2
CHADS
2
score was superior to the CHADS
2
and
CHA
2
DS
2
-VASc scores in predicting LA/LAA thrombosis.
AF is an independent risk factor for thromboembolic stroke
and peripheral emboli. One of the key steps in preventing
stroke associated with AF is effective risk stratification to guide
decision making with regard to the need for anticoagulant
therapy.
20
The CHADS
2
score is commonly used for this risk
stratification in patients with AF. The CHA
2
DS
2
-VASc score
was recommended by the European Society of Cardiology and
the American College of Cardiology (ACC)/American Heart
Association (AHA) guidelines in 2012 and 2014, respectively,
for stroke risk stratification in NVAF patients.
21-23
However, these
two score systems have been criticised.
19
Yarmohammadi
et al
.
24
reported in a substudy of the ACUTE
trial that the CHADS
2
score could not reliably predict embolic
risk in patients with NVAF because 10% of the patients ranked
with zero points had LA thrombi. Fruhauf
et al.
25
also reported a
case involving a NVAF patient who had CHADS
2
and CHA
2
DS
2
-
VASc scores of zero points; this patient then developed recurrent
LAA thrombi after radiofrequency catheter ablation. Therefore,
although the current stroke risk-stratification schemes appear to
be practical, they still have some defects and limitations.
We found that patients with non-chicken wing LAA
morphology had a significantly higher risk of LA/LAA
thrombosis compared with chicken wing morphology. The
chicken wing morphology was the most common LAA form
(67.9%) in our population and the least associated with a history
of LA thrombosis, which was in accordance with the Di Biase
et al.
studies.
7
To date, there have been no data incorporating
LAA morphology into stroke risk stratification.
Our data indicated that LAA morphology remained the
most powerful independent predictor of LA/LAA thrombosis
with multivariable regression analysis (OR: 11.48; 95% CI:
4.157–31.684; p = 0.000). According to Clark
et al
., the CHADS
2
risk score was the most commonly used scoring system for the
evaluation of stroke risk.
19
We found that there were 27 subjects
(77.1%) with a CHADS
2
score of zero or one in the thrombus
group but they all developed a LA/LAA thrombus. Of these 27
individuals, 23 (85.2%) had non-chicken wing LAA and only
four (14.8%) had chicken wing LAA. Moreover, there were 84
subjects (16.2%) with a CHADS
2
score of two points or more
in the non-thrombus group. In these 84 cases, 55 (65.5%) had
chicken wing LAA and 29 (34.5%) had non-chicken wing
LAA. This suggested that LAA morphology might be useful
for predicting the risk of thromboembolism in NVAF patients
with low and high CHADS
2
scores (Tables 1, 3). We therefore
incorporated LAA morphology (L with highest points of two)
into the CHADS
2
score, leading to the L
2
CHADS
2
risk score.
The utility of the L
2
CHADS
2
score for predicting risk
of systemic emboli, as indicated by the results of the AUC
calculation, was higher than that of either the CHADS
2
or CHA
2
DS
2
-VASc scores. These results indicated that the
L
2
CHADS
2
score was superior to either the CHADS
2
or the
CHA
2
DS
2
-VASc scores for predicting LA thrombus formation.
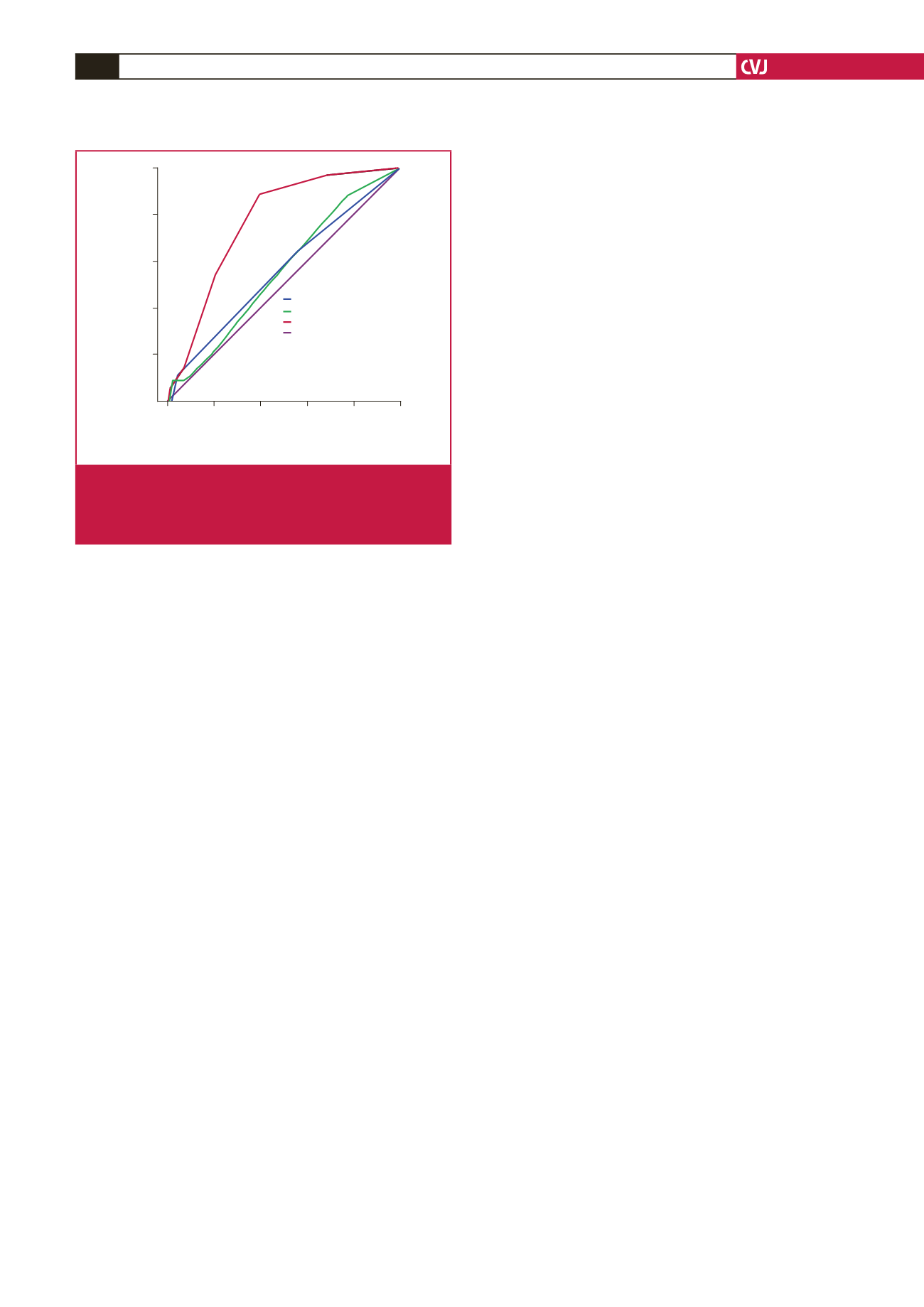
The CHADS
2
score had high specificity but poor sensitivity (Fig.
5). This led to missed opportunities for anticoagulant therapy for
a majority of patients with a high risk of stroke. The CHA
2
DS
2
-
VASc score increased the sensitivity at the cost of reducing
specificity to 0.225. This observation was in agreement with the
USA
26
and Portuguese
27
TEE and European clinical outcomes
studies.
11,28-30
On the other hand, compared to the CHADS
2
score,
the L
2
CHADS
2
score had higher sensitivity and specificity (0.427
and 0.606, respectively). These observations suggested that the
L
2
CHADS
2
score could identify ‘truly low-risk’ patients without
sacrificing overall predictive ability. Therefore the findings were
consistent in showing the advantage of the L
2
CHADS
2
risk score.
The risk for stroke may be balanced by the risk of bleeding,
which can be a deadly complication in patients with NVAF who
are treated with anticoagulants.
23
The 2016 AHA/ACC guidelines
pointed out that patients with NVAF and a CHA
2
DS
2
-VASc
score of one point, taking aspirin or anticoagulant drugs or not
taking any medications (Class IIb, C), had similar outcomes.
That is to say, the clinical decision making is still controversial
in patients with intermediate risk.
31
The CHADS
2
score has
been criticised for categorising a great number of patients with
NVAF as intermediate risk.
32
Compared with the CHADS
2
score,
the CHA
2
DS
2
-VASc and L
2
CHADS
2
scores placed a smaller
percentage of patients in the intermediate-risk group; there was
a reduction to 43 (18.8%) and 73 (31.9%) patients, respectively.
Because the L
2
CHADS
2
score reduced these percentages to a
greater extent, utilising it may reduce uncertainties about the
benefits of anticoagulant therapy in patients with intermediate
risk.
Our data revealed that for NVAF subjects who had LA
thrombus on TEE, more than two-thirds developed these clots
despite having a low CHADS
2
score of zero or one point. This
suggested that a high proportion of patients with high risk of
Source of
the curve
1.0
0.8
0.6
0.4
0.2
0.0
0.0
0.2
0.4
0.6
0.8
1.0
1 - Specificity
Sensitivity
Diagonal segments are produced by ties
CHADS
2
CHA
2
DS
2
-VASc
LAA
Reference line
Fig. 5.
Receiver operating characteristic (ROC) curves for
the prediction of LA/LAA thrombus by the CHADS
2
,
CHA
2
DS
2
-VASc and L
2
CHADS
2
risk-stratification
schemes. AUC, area under the curve.