CARDIOVASCULAR JOURNAL OF AFRICA • Vol 21, No 5, September/October 2010
272
AFRICA
Dually noted, Africans are usually salt sensitive and reveal
sympathetic over-activity, and this could probably be the link
between the aforementioned mechanism and augmented preva-
lence of hypertension in Africans.
11,27
As the AC men were not
centrally obese, the latter explanation of inherent enhanced
sympathetic activity
11
and subsequent increased MS indicators
could rather contribute to the strong associations found between
dyslipidaemia, impaired fasting glucose and sub-clinical athero-
sclerosis, as well as renal impairment.
The HDL findings in AC men are of major significance,
as HDL levels correlated negatively with blood pressure and
sub-clinical atherosclerosis, which is indicative of atherogenic
dyslipidaemia, found in both type 2 diabetes and the MS.
13
Ultimately, dyslipidaemia could result in coronary heart disease,
supporting the fact that the MS and its underlying factors are
the most important risk factors for myocardial infarction.
13,18
The
lower cholesterol values in AC men compared to PC men were
positively associated with CIMT
f
, which is difficult to explain, as
this clearly contradicts literature regarding the role of cholesterol
and development of sub-clinical atherosclerosis
11, 13,16-18,28
Clearly,
more research is needed on this topic.
Africans and African-Americans are collectivistic population
groups, who view the experience of social support from their
extended families as important, and social support possibly has
a protective effect on their cardiovascular status.
29
Social support
in the PC men though, contributed significantly to augmented
CIMT (
r
=
0.53). PC has been implicated in depression.
Therefore, it could be that these PC men had already reached
avoidance, withdrawal and depression, to the point that social
support became a stress factor, rather than a way of coping.
12
Both hypotheses were accepted as, firstly, utilising an AC
style was associated with increases in MS indicator values in
urban African men. Secondly, a synergistic effect was illustrated
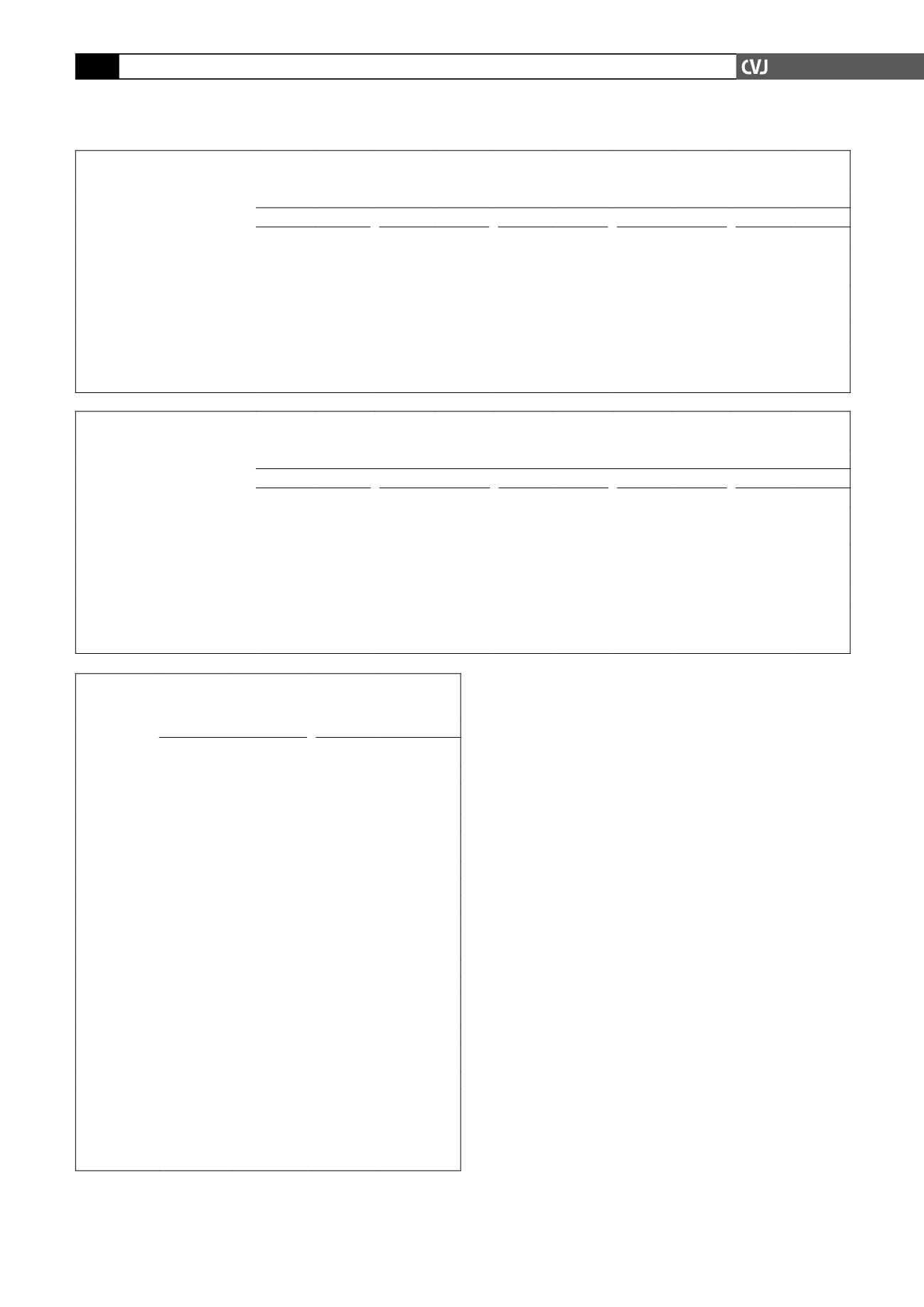
TABLE 2. PARTIAL CORRELATIONS OF MSAND TARGET END-ORGAN DAMAGE INDICATORS IN URBANACTIVE COPING
BLACK MEN, INDEPENDENT OFALCOHOL CONSUMPTION
19
Active coping (
n
=
30)
SBP (mmHg)
DBP (mmHg)
Glucose (mmol/l)
TG (mmol/l)
CIMT
f
(mm)
r
p
r
p
r
p
r
p
r
p
Glucose (mmol/l)
0.324 0.086
0.273 0.152 1.000
–
0.301 0.070
0.633 0.000
TG (mmol/l)
0.215 0.201 0.121 0.533 0.243 0.203 1.000
–
0.215 0.262
HDL (mmol/l)
–0.455 0.013 –0.402 0.031
–0.263 0.169 –0.262 0.171
–0.488 0.007
WC (cm)*
–
–
–
–
–
–
–
–
–
–
Microalbuminuria (
µ
g/l/min)
0.065 0.736 –0.022 0.911
0.499 0.006 0.564 0.001
0.348 0.065
MS: metabolic syndrome;
n
, number of subjects; SBP: systolic blood pressure; DBP: diastolic blood pressure; TG: triglycerides; HDL: high-
density lipoproteins; CIMT
f
: carotid intima–media thickness far wall. All values in bold with
r
≥
0.350 and
p
≤
0.05 differ significantly, and values
in bold italics are borderline significant. *WC: waist circumference data presented in Fig. 1.
TABLE 3. PARTIAL CORRELATIONS OF MSAND TARGET END-ORGAN DAMAGE INDICATORS IN URBAN PASSIVE COPING
BLACK MEN, INDEPENDENT OFALCOHOL CONSUMPTION
19
Passive coping (
n
=
23)
SBP (mmHg)
DBP (mmHg)
Glucose (mmol/l)
TG (mmol/l)
CIMT
f
(mm)
r
p
r
p
r
p
r
p
r
p
Glucose (mmol/l)
0.097 0.676 0.207 0.368 1.000
–
0.188 0.414 –0.044 0.850
TG (mmol/l)
0.083 0.720 0.279 0.221 0.188 0.414 1.000
–
–0.259 0.257
HDL (mmol/l)
–0.103 0.658 –0.096 0.679 –0.164 0.478
–0.525 0.014
0.124 0.591
WC (cm)*
–
–
–
–
–
–
–
–
–
–
Microalbuminuria (
µ
g/l/min)
0.773 0.000 0.710 0.000
0.137 0.554 –0.007 0.977 0.207 0.368
MS: metabolic syndrome;
n
: number of subjects; SBP: systolic blood pressure; DBP: diastolic blood pressure; TG: triglycerides; HDL: high-
density lipoproteins; CIMT
f
: carotid intima–media thickness far wall. All values in bold with
r
≥
0.350 and
p
≤
0.05 differ significantly, and values
in bold italics are borderline significant. *WC: waist circumference data presented in Fig. 2.
TABLE 4. MULTIPLE FORWARD STEPWISE REGRESSIONANALYSES
INDICATING INDEPENDENTASSOCIATIONS BETWEEN MEASURES OF
MSAND TARGET END-ORGAN DAMAGE INDICATORS
Urban AC African men (
n
=
30) Urban PC African men (
n
=
23)
CIMT
f
(mm)
Microalb
(
µ
g/l/min)
CIMT
f
(mm)
Microalb
(
µ
g/l/min)
Adjusted
r
2
0.547
0.606
0.588
0.665
Independent
variables
β
(SE)
β
(SE)
β
(SE)
β
(SE)
Age (years)
–
–
0.627 (0.15)
§
–
Body mass index
(kg/m
2
)
–
–
–
–
Alcohol (%)
–
–
0.513 (0.15)*
–
Smoking (%)
–
–
–
–
PAI-3 (kcal/24 h)
–
0.404 (0.13)*
–
–
Social support
–
–
0.531 (0.14)*
–
Cholesterol
(mmol/l)
0.407 (0.17)**
–
–
–
SBP (mmHg)
–
–
–
0.596 (0.26)**
DBP (mmHg)
–
–0.360 (0.14)**
–
0.442 (0.28)
Waist circum-
ference (cm)
–
0.789 (0.22)
§
–
–0.408 (0.16)**
Glucose (mmol/l)
0.482 (0.14)
§
0.354 (0.13)*
–0.282 (0.16)
–
Triglycerides
(mmol/l)
–0.236 (0.16)
0.378 (0.13)*
–
–
HDL (mmol/l)
–0.554 (0.16)
§
0.373 (0.18)
–
–
MS: metabolic syndrome indicators; AC: active coping;
n
: number of participants;
CIMT
f
: carotid intima–media thickness far wall; Microalb: microalbuminuria log
transformed;
β
: beta coefficient, SE: standard error; PAI-3: high physical activity;
SBP: systolic blood pressure; DBP: diastolic blood pressure; HDL: high-density lipo-
proteins. Values in bold and with the same superscripts differ significantly:
§
p
≤
0.004;
*
p
≤
0.01; **
p
≤
0.05, and values in bold italics are borderline significant.


