CARDIOVASCULAR JOURNAL OF AFRICA • Vol 24, No 4, May 2013
118
AFRICA
the cause of heart disease was not recorded. One hundred and
fifty-eight cases (91 males, 67 females) were analysed.
Diagnosis was made on the basis of symptoms and signs. In
infants, these were feeding difficulties, increased fatiguability,
tachynoea, intercostal retraction, dysponoea, grunting,
tachycardia, gallop rhythm, cyanosis, rales and hepatomegaly.
In older children, the symptoms and signs included exercise
intolerance, somnolence, anorexia, tachypnoea, dyspnoea,
orthopnoea, cough, wheezing, rales, gallop rhythm, oedema,
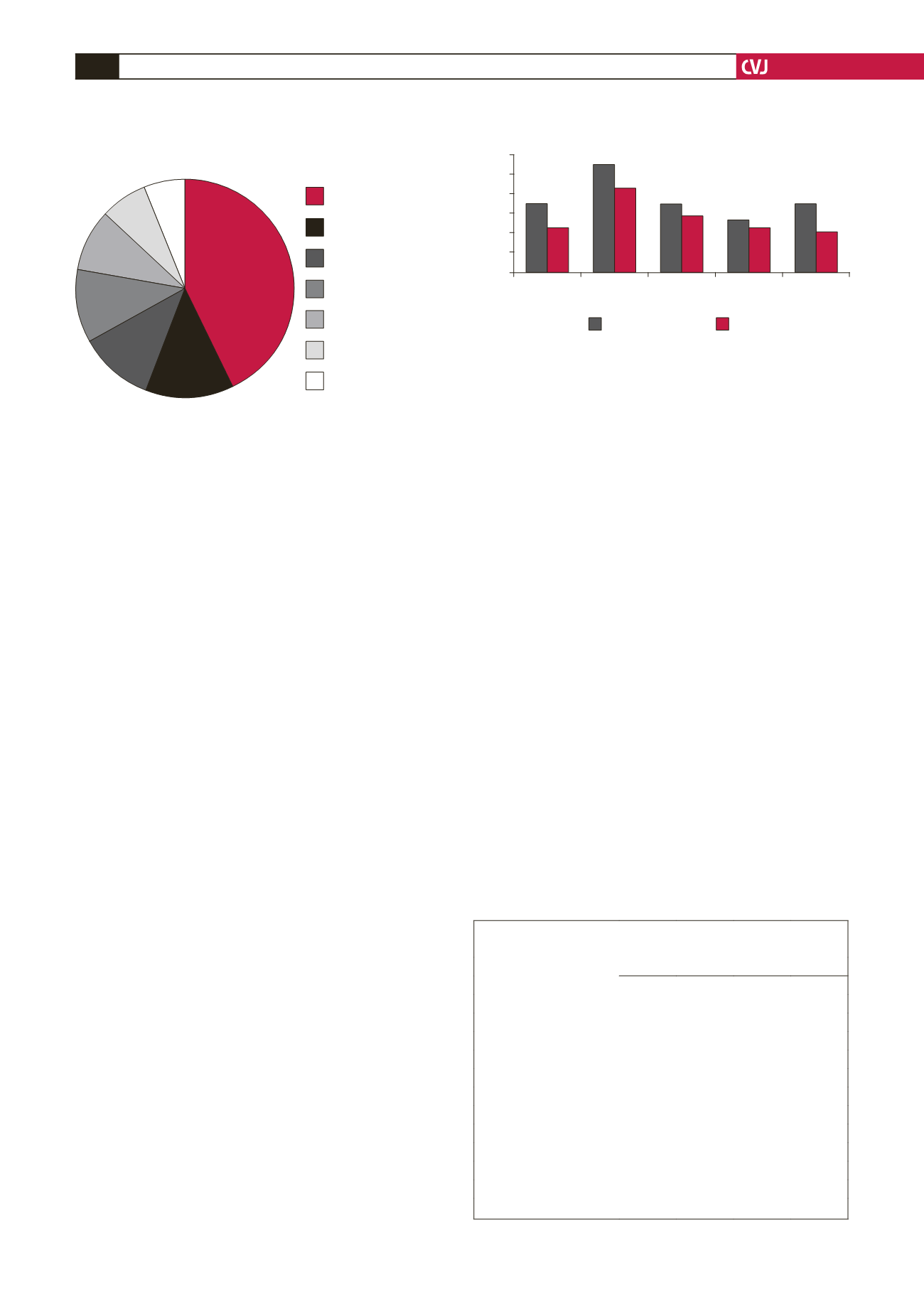
hepatomegaly, and raised jugular venous pressure. The most
common investigations used to complement clinical diagnosis
were echocardiography combined with ECG (43.0%), and echo
alone (12.6%). Echo, ECG and CXR were done in 11.4 %, and
ECG alone in 10.8% (Fig. 1).
Routine laboratory tests done for all patients included total
blood count (TBC), peripheral blood film (PBF), and urea,
electrolytes and creatinine (U/E/Cs) levels. Specific tests done
were brain natriuretic peptide (BNP) (12.6%), C-reactive protein
(CRP) (11.4%), tumour necrotic factor (TNF) alpha (11.4%),
human immunodeficiency virus (HIV) ELISA (13.8%), CD
4
counts (13.8%), and blood cultures (13.3%). The Mantoux test
was done in those suspected to have tuberculosis.
The mean age of these patients was 4.7 years, peaking at
1–3 years (range: 2 months – 12 years). The male:female ratio
was 1.4:1, and the male predominance persisted through all age
groups (Fig. 2).
The most common single cause was infections (22.8%).
Among these, the infections recorded were pneumonia (50%),
upper airway (19.4%), throat (16.7%), and urinary tract (13.9%)
infections. Anaemia (17.1%) was the second most common
cause. The anaemia was due to malaria (48.2%), helminthiasis
(22.2%), malnutrition (14.8%), and sickle cell disease (14.8%).
Other causes included rheumatic (14.6%) and congenital (13.3%)
heart disease, cardiomyopathy (7.6%), tuberculosis and HIV
(6.9%) (Table 1).
Eleven (7.0%) of the cases had multiple causes; six more
than one, and five more than two. In six cases (3.8%), HIV was
combined with tuberculosis. In five cases (3.2%), there were
more than two causes: three in which bacterial infection was
combined with cardiomyopathy and HIV, and two in which there
was malaria, anaemia and infection.
Treatment comprised appropriate correction of cause of heart
failure, such as treatment of infection with antibiotics, blood
transfusion and haemantics to treat anaemia, and correction
of malnutrition with nutritional supplements. Heart failure
was treated with diuretics,
β
-blockers, angiotensin converting
enzyme (ACE) inhibitors and digoxin in various combinations.
Successful surgical correction was done on 11 of those with
CHD (7.6%) and 10 of those with RHD (6.3%). The remaining
23 cases of CHD and RHD (14.5%) were referred to other
centres for surgery and were lost to follow up. Overall, 77.9% of
patients recovered and only 7.6% died while in hospital.
Discussion
Observations of the current study reveal that heart failure
constitutes about 1:1 000 of paediatric hospital admissions. It
is difficult to compare rates among hospitals due to different
hospital sizes, paediatric age limit, diagnostic criteria, age
distribution and profile of causes.
The modes of diagnosis combining clinical symptoms,
signs and investigations are concordant with those practiced
elsewhere.
9,10
This implies that detection rates are comparable to
those in other centres. Accordingly, any differences may result
from other factors, probably related to age and cause.
The mean age at presentation was 4.7 years, comparable
to the 3.7
±
3.5 years reported from Nigeria.
2
Notably, this is
beyond infancy and is commensurate with observations that
congenital defects constitute less than acquired causes of heart
failure. In developed countries where congenital heart disease
is the leading cause,
1,9,11
the mean age is much lower. The mean
age is also affected by one-year survival rates and is dependent
TABLE 1. DISTRIBUTION OF CAUSESAMONG CONGESTIVE
HEART FAILURE PAEDIATRIC PATIENTS
Cause
Distribution
Male Female Total
%
Infections
20
16
36
22.8
Anaemia
17
10
27
17.1
Rheumatic heart disease
12
11
23
14.6
Congenital heart disease
10
11
21
13.3
Cardiomyopathy
5
7
12
7.6
Tuberculosis
5
6
11
6.9
HIV
8
3
11
6.9
Adenoid hypertrophy
2
1
3
1.9
Rickets
1
2
3
1.9
More than one cause
6
0
6
3.8
More than two causes
5
0
5
3.2
Total
91
67
158
100
Mode(s) of diagnosis
43%
13%
11%
11%
9%
7%
6%
ECG and echo
Echocardiography
(echo) alone
Chest X-ray,
ECG and echo
Electrocardiography
(ECG) alone
Chest X-ray alone
Chest X-ray and ECG
Chest X-ray and echo
Fig. 1. Modes of diagnosis of paediatric heart failure.
Fig. 2. Gender distribution by age.
30
25
20
15
10
5
0
< 1 year
1–3 years 4–6 years 7–9 years 10–12 years
Number of patients
Age category
Male
Female


