
















 61 / 78
61 / 78

CARDIOVASCULAR JOURNAL OF AFRICA • Volume 26, No 4, July/August 2015
AFRICA
e7
biventricular hypertrophy. A chest radiograph revealed marked
cardiomegaly with a prominent main pulmonary trunk and
increased pulmonary vascularity.
Transthoracic echocardiography indicated a levocardia
heart with atrial situs solitus and concordant atrioventricular
connections. Marked biventricular hypertrophy in the four-
chamber view was also evident. The left ventricle demonstrated
a normal ejection fraction. The most striking finding was a
single large vessel arising from the base of the heart, with mild
regurgitation related predominantly to the summit of the right
ventricle (70%). A large, non-restrictive outlet VSD was noted
beneath the truncal valve (Fig. 1). Neither the pulmonary artery
(PA) nor the pulmonary valve could be seen.
Cardiac MRI was also performed to better delineate the
origin of the pulmonary arteries. It demonstrated a dilated
common arterial trunk with the left and right pulmonary arteries
arising from a short main pulmonary trunk at the posterior
side of the common arterial trunk. The left ventricle (LV) was
normal in size. The right ventricle (RV) was also normal in
size with concentric hypertrophy. A large, subarterial VSD was
noted beneath the truncal valve, which was trileaflet, with mild
insufficiency (Fig. 2).
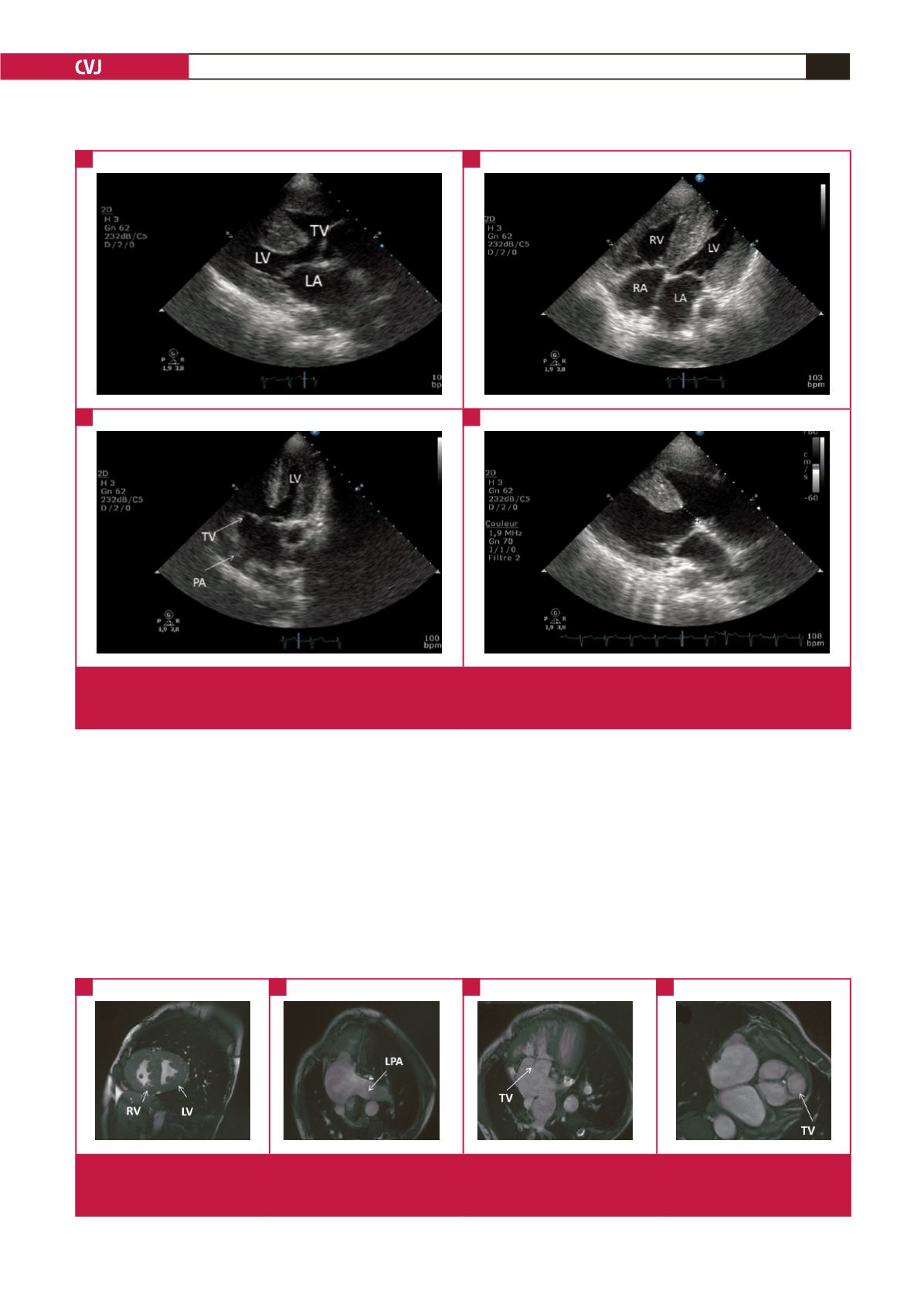
Fig. 1.
Transthoracic echocardiogram revealed a hypertrophied right ventricle, a single great vessel (persistent truncus arteriosus)
overriding both ventricles, and a large single subtruncal ventricular septal defect. LA, left atrium; RA, right atrium; LV, left
ventricle; RV, right ventricle; TV, troncal valve; PA, pulmonary artery.
A
C
B
D
Fig. 2.
MRI demonstrated a dilated common arterial trunk with the left and right pulmonary arteries arising from a short main
pulmonary trunk at the posterior side of the common arterial trunk. LV, left ventricle; RV, right ventricle; TV, troncal valve;
LPA, left pulmonary artery.
A
C
B
D