
















 65 / 72
65 / 72

CARDIOVASCULAR JOURNAL OF AFRICA • Volume 27, No 2, March/April 2016
AFRICA
119
Assessing perinatal depression as an indicator of risk
for pregnancy-associated cardiovascular disease
Lauren Nicholson, Sandrine Lecour, Sonja Wedegärtner, Ingrid Kindermann, Michael Böhm, Karen Sliwa
Abstract
Cardiovascular conditions associated with pregnancy are seri-
ous complications. In general, depression is a well-known risk
indicator for cardiovascular disease (CVD). Mental distress
and depression are associated with physiological responses
such as inflammation and oxidative stress. Both inflammation
and oxidative stress have been implicated in the pathophysiol-
ogy of CVDs associated with pregnancy. This article discusses
whether depression could represent a risk indicator for CVDs
in pregnancy, in particular in pre-eclampsia and peripartum
cardiomyopathy (PPCM).
Keywords:
cardiovascular disease in pregnancy, peripartum
cardiomyopathy, depression in pregnancy
Submitted 19/8/15, accepted 14/11/15
Cardiovasc J Afr
2016;
27:
119–122
www.cvja.co.zaDOI: 10.5830/CVJA-2015-087
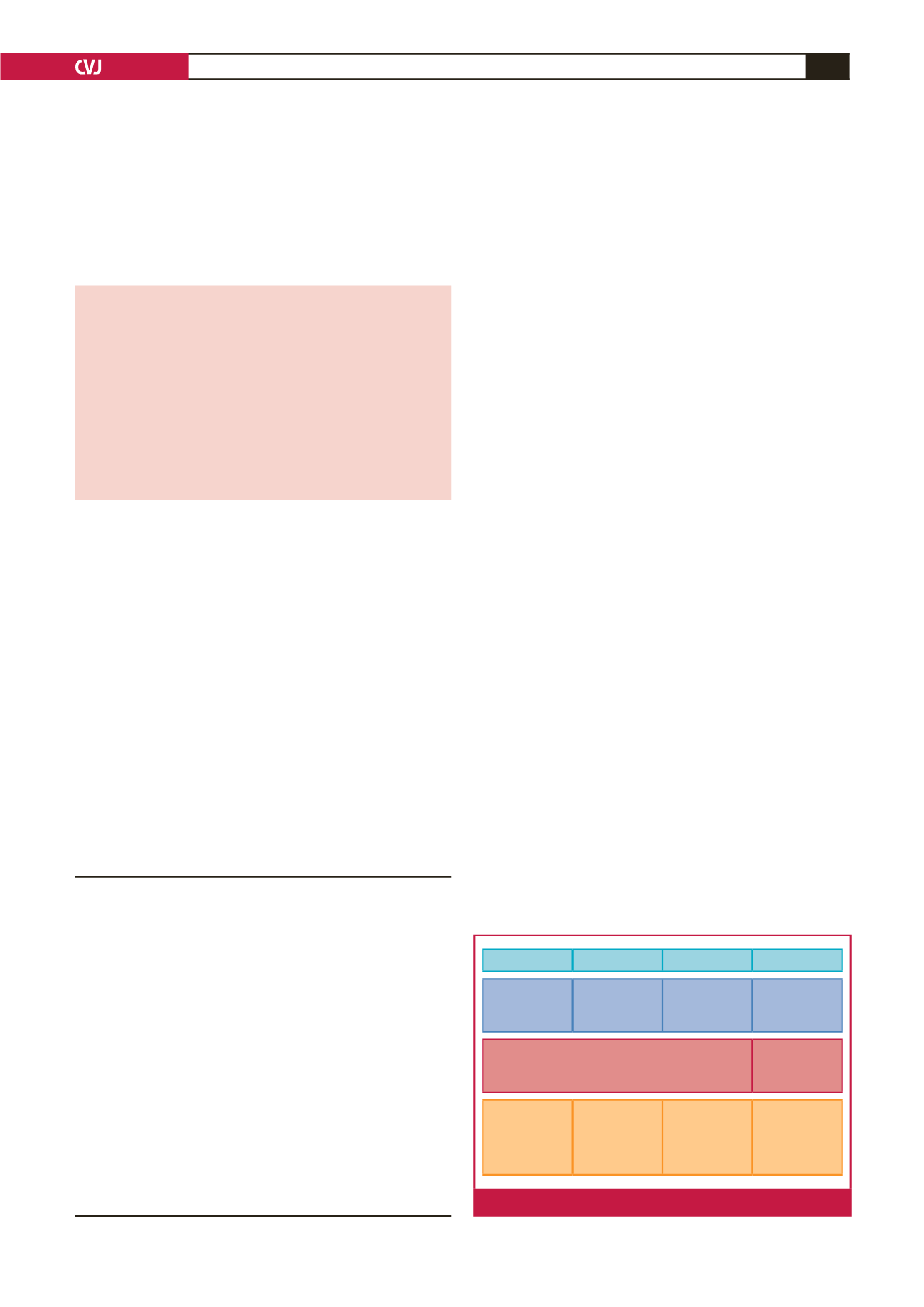
The physiological changes associated with pregnancy, such as
increased oxidative stress and circulatory changes, place a burden
on the cardiovascular system of pregnant women (Fig. 1).
1
Cardiovascular conditions associated with pregnancy, such as
peripartum cardiomyopathy (PPCM) and pre-eclampsia, could
result in serious cardiovascular complications.
2,3
Psychosocial factors, for example depression, are increasingly
being recognised as risk indicators for cardiovascular diseases
such as ischaemic heart disease.
4
Mental disorders such as
anxiety and depression are the third leading burden of disease
in women globally.
5
Women of childbearing age have the highest
prevalence of psychiatric disorders, in particular, anxiety and
mood disturbances.
6,7
Previous studies have explored the association between
depression and cardiovascular disease (CVD),
4,8
and have
demonstrated that depression is a risk factor for CVD and
increases both morbidity and mortality rates.
8
This article
discusses the potential contribution of depression during the
peripartum period to the pathophysiology of CVD in pregnancy.
Physiological adaptations in pregnancy
Major compensatory changes are made by the maternal heart
to accommodate the demands of pregnancy and lactation.
9
In
pregnancy, the foreign material of the foetus is not rejected by the
maternal immune system,
10
as increased oxidative stress during
the first trimester prevents this rejection.
11
During pregnancy
women experience a reversible adaptive cardiac hypertrophy
(Fig. 1) and reduced relaxation of diastolic function, whereas in
healthy women this regresses to normal following childbirth.
12
Increase in oxidative stress during pregnancy
In the first trimester, oxidative stress, which is an increased
production of reactive oxygen species compared to anti-
oxidant defence mechanisms,
13
regulates the invasion of foreign
trophoblastic material in the maternal body.
11
These oxidative
stress mechanisms also control normal and pathological
embryogenesis.
14
The hormone oestrogen mediates regulation of
the balance between pro-oxidative and anti-oxidative molecules
guarding this process.
14
An increase in oxidative stress during pregnancy can be
characterised by enhanced lipid peroxidation and the circulation
of lipid hydroperoxides.
14
The increase in oxidative stress in
healthy women peaks around the second trimester.
15
When
Hatter Institute for Cardiovascular Research in Africa and
MRC Inter-University Cape Heart group, Department of
Medicine, University of Cape Town, South Africa
Lauren Nicholson, BSc (Med), Hons, MSc (Med), nchlau002@
myuct.ac.zaSandrine Lecour, PhD, DPharm
Hatter Institute for Cardiovascular Research in Africa, and
IDM, Department of Medicine, Faculty of Health Sciences,
University of Cape Town, South Africa; Soweto Cardiovascular
Research Unit, University of the Witwatersrand,
Johannesburg; Inter-Cape Heart Group, Medical Research
Council South Africa, Cape Town, South Africa
Karen Sliwa, MD, PhD, FESC,
karen.sliwa-hahnle@uct.ac.zaClinic for Internal Medicine III, Cardiology, Angiology and
Intensive Care Medicine, University Hospital of Saarland,
Homburg/Saar, Germany
Sonja Wedegärtner, Dip (Psychol)
Ingrid Kindermann, PhD (Med)
Michael Böhm, MD, FESC
1st Trimester 2nd Trimester 3rd Trimester 4th Trimester
Increase in
oxidative stress
Oxidative stress
levels peak
Oxidative stress
decreases
Oxidative stress
normalises
Inflammatory
cascade
Suppression of
maternal innate
and adaptive
immune
response
Suppression of
maternal innate
and adaptive
immune
response
Immune function
normalises
Reversible cardiac hypertrophy
Normal cardiac
function
Fig. 1.
The physiological changes associated with pregnancy.