
















 28 / 80
28 / 80

CARDIOVASCULAR JOURNAL OF AFRICA • Volume 28, No 3, May/June 2017
162
AFRICA
acylated ghrelin and saliva levels of obestatin were higher. In our
previous study, we found that saliva levels of both parameters
were higher than the serum levels in both groups.
22
The high ghrelin and obestatin levels found in saliva are very
likely a consequence of the function of the salivary gland, since
obestatin is produced by this gland. Both our own research team
22
and Gröschl
et al.
32
have previously independently reported that
the salivary gland produces its own ghrelin.
In our previous study,
4
we attributed the significantly higher
saliva levels of ghrelin and obestatin, in comparison to serum
levels, to the fact that they had undergone greater degradation
in the blood due to pre-analysis errors, such as the temperature
of collection and centrifugation. In the present study, when the
serum and saliva levels of these peptides were compared between
groups, it was found that serum ghrelin levels were elevated while
serum obestatin levels were reduced in the patients with IHD,
compared to the control group. We believe that these elevated
ghrelin levels occur in order to curtail ischaemic heart damage.
In a study conducted by Laurila
et al.
,
33
high plasma ghrelin
concentration was correlated with protection from coronary
heart disease. Sax
et al.
found that pericardial active ghrelin
concentration and the pericardial-to-plasma ghrelin ratio were
elevated in IHD patients, compared to non-ischaemic subjects,
and suggested an increased ghrelin production by the chronically
ischaemic myocardium.
34
Gnanapavan
et al.
demonstrated
mRNA expression of ghrelin in the myocardium and veins. They
determined that GHS-R1a was expressed in the myocardium and
not the veins, while GHS-R1b was expressed in both.
25
On the
basis of these studies, it can be asserted that ghrelin is a critical
peptide for the cardiovascular system.
Li
et al.
examined the role of pro-inflammatory cytokines,
reporting that ghrelin may inhibit the TNF-
α
-induced IL-8
release in a concentration-dependent manner.
11
Mononuclear
cell adhesion molecules are an integral part of vascular
inflammation and atherosclerosis, as induced by chemotactic
cytokines. Ghrelin inhibits the activity of nuclear factor kappa
B (NF-
κ
B), which is crucial in the production of chemotactic
cytokines, and adhesion molecule expression, which adversely
affects endothelial cell response.
11
Ghrelin has also been shown to
improve left ventricular function in heart failure.
35,36
In addition, ghrelin’s mechanism of action on endothelial
cells may be linked to GHS-R, a seven-transmembrane G
protein-coupled ghrelin receptor. Stimulation of GHS-R with
ghrelin leads to activation of G protein, calcium mobilisation
and multiple downstream signalling.
37
Ghrelin receptors have
been isolated in various tissues, such as the endocrine glands and
cardiovascular tissue. In addition, receptor density changes have
been demonstrated to be an important part of the cardiovascular
effects of ghrelin.
38
Ghrelin has also been reported to prevent
apoptosis in cardiac cells.
8
An inverse correlation was found between serum total ghrelin
levels and systolic blood pressure in our study. Studies reporting
that ghrelin significantly reduced mean arterial blood pressure
confirm our results.
35,39,40
In this study, both patients and controls had a mean BMI
higher than that considered normal worldwide, although they
are not regarded as obese. The mean BMI for the patients in
the study was 25.5
±
3.4 kg/m
2
, which is classified as overweight.
Therefore, the BMIs of the controls (25.1
±
3.1 kg/m
2
) were
matched to those of the patients. If the BMIs of the controls
and patients had not been matched, it may have influenced
obestatin and ghrelin secretion independent of the heart disease,
as an increase in ghrelin level has been correlated with a decrease
in body weight.
41
A weakly negative correlation was also found
between the serum acylated ghrelin and BMI in the IHD
subjects, but there was no correlation in the controls. Several
previous studies support our findings.
22,32,41,42
Aydin assumed that low serum levels of obestatin also served
to reduce ischaemic damage, as obestatin and ghrelin counteract
one another.
13
However, given that an elevated saliva obestatin
level is only related to the circulation via transport from blood
to saliva, and that the salivary gland also secretes obestatin, it is
presumed that the elevated saliva level may have resulted from
the contribution of this gland.
2
Inaddition, Iglesias andcolleagues recently found that obestatin
had no effect on cardiomyocyte viability and metabolism.
43
The
pathophysiological role of obestatin in ischaemic heart disease
therefore remains an important research topic.
Salivary Hcy levels in both groups were found to be
significantly lower than serum levels in our study. A possible
explanation for this is that Hcy, which is a very weak lipophilic
molecule, is bound to plasma proteins in large amounts, with
the result that its diffusion to saliva is reduced. In routine
clinical chemistry, the measured salivary components diffuse
into the saliva from the blood. It has been reported that several
factors play a part in the diffusion of serum components, such
as Hcy, into saliva, namely that lipophilic components diffuse
more easily than lipophobic components, the rate of ionised
components in the saliva to those in the plasma changes with
salivary pH, and the binding of components to proteins is a
crucial factor in this rate.
44
While there was no significant difference between the salivary
Hcy levels of the control and IHD groups, serum Hcy levels were
found to be significantly higher in IHD patients. One reason why
serum Hcy levels increase in IHD is believed to be a deficiency
of vitamin B
12
and folic acid, which function as co-factors and
co-substrates in Hcy metabolism.
45,46
Serum levels of B
12
and folic
acid, which act in the pathway of the Hcy metabolism, were also
found to be significantly lower in the patient group in our study.
An elevated Hcy level is considered to be a risk factor for
the development of atherosclerosis. It has been suggested that
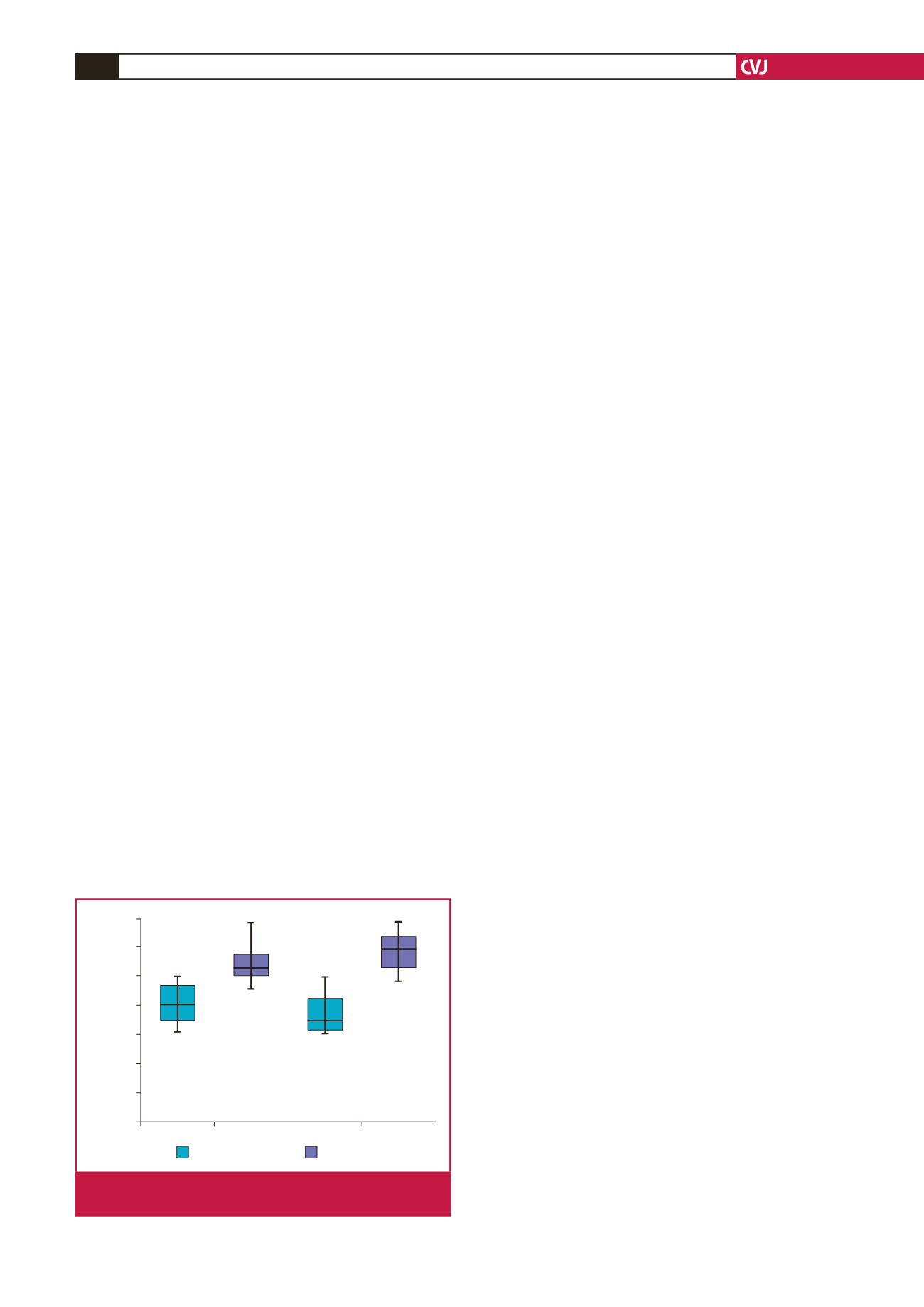
Control
IHD
700
600
500
400
300
200
100
0
Obestatin (pg/ml)
Obestatin serum
Obestatin saliva
Fig. 3.
Serum and saliva obestatin levels of controls and
patients with ischaemic heart disease.