
















 71 / 80
71 / 80

CARDIOVASCULAR JOURNAL OF AFRICA • Volume 28, No 3, May/June 2017
AFRICA
e1
Case Report
Persistent left superior vena cava
Kamil W Tyrak, Jakub Hołda, Mateusz K Hołda, Mateusz Koziej, Katarzyna Pi
ą
tek, Wiesława Klimek-
Piotrowska
Abstract
Persistent left superior vena cava (PLSVC) is the most
common congenital malformation of thoracic venous return
and is present in 0.3 to 0.5% of individuals in the general
population. This heart specimen was dissected from a 35-year-
old male cadaver whose cause of death was determined as
non-cardiac. The heart was examined and we found a PLSVC
draining into the coronary sinus. The right superior vena cava
was present with a small-diameter ostium. An anomalous
pulmonary vein pattern was observed; there was a common
trunk to the left superior and left inferior pulmonary veins
(diameter 17.8 mm) and an additional middle right pulmo-
nary vein (diameter 2.7 mm) with two classic right pulmonary
veins. The PLSVC draining into the coronary sinus had led to
its enlargement, which could have altered the cardiac haemo-
dynamics by significantly reducing the size of the left atrium
and impeding its outflow via the mitral valve.
Keywords:
coronary sinus, persistent left superior vena cava, right
atrium, left atrium
Submitted 17/4/16, accepted 15/9/16
Cardiovasc J Afr
2017;
28
: e1–e4
www.cvja.co.zaDOI: 10.5830/CVJA-2016-084
Persistent left superior vena cava (PLSVC) is the most common
congenital malformation of the thoracic venous return and is
present in 0.3 to 0.5% of individuals in the general population
with a normal heart, and 4.5% in individuals with congenital
heart diseases.
1
A PLSVC co-occurs with the right superior vena
cava in 80 to 90% of cases,
2
and may also be accompanied by
other heart abnormalities, such as anomalous connections of
the pulmonary veins, aortic coarctation, tetralogy of Fallot,
transposition of the great vessels as well as dextroversion.
1,3,4
Moreover, cardiac rhythm disturbances concerning impulse
formation and conduction have been observed.
The PLSVC usually drains into the right atrium (in 80–92%)
through a dilated coronary sinus (CS),
5,6
but in approximately 10
to 20% of cases, it is associated with left atrial (LA) drainage.
7,8
The PLSVC may drain directly through the left atrium or via the
unroofed CS, which is a cause of right-to-left cardiac shunt. The
majority of patients with PLSVC are asymptomatic. In general,
only patients with unusual drainage and right-to-left shunting are
of clinical significance. Anomalous venous return via the PLSVC
may be the cause of cardiac arrhythmias, decreased exercise
tolerance, progressive fatigue, chest discomfort, palpitations,
syncope or cyanosis.
6
The implications of existing PLSVC could be important for
clinicians who are involved in placement of central venous-access
devices.
9
Access to the right side of the heart or pulmonary
vasculature through the left subclavian vein is much more
difficult in patients with PLSVC. Placement of a central line
or cardiac resynchronisation therapy leads and pacemaker
implantation in undiagnosed cases with PLSVC can result in
incorrect positioning.
10
In those cases, access to the right heart
and coronary sinus should be performed via the right subclavian
vein, allowing for an easier route. Also the presence of PLSVC
is a relative contraindication to the administration of retrograde
cardioplegia during cardiac surgery.
6
Case report
This heart specimen was dissected from a 35-year-old male
cadaver (BMI 29.9 kg/m
2
) whose cause of death was determined
Department of Anatomy, Jagiellonian University Medical
College, Cracow, Poland
Kamil W Tyrak,
kamiltyrak@gmail.comJakub Hołda
Mateusz K Hołda, PhD
Mateusz Koziej, MD
Katarzyna Pi
ą
tek
Wiesława Klimek-Piotrowska, MD, PhD
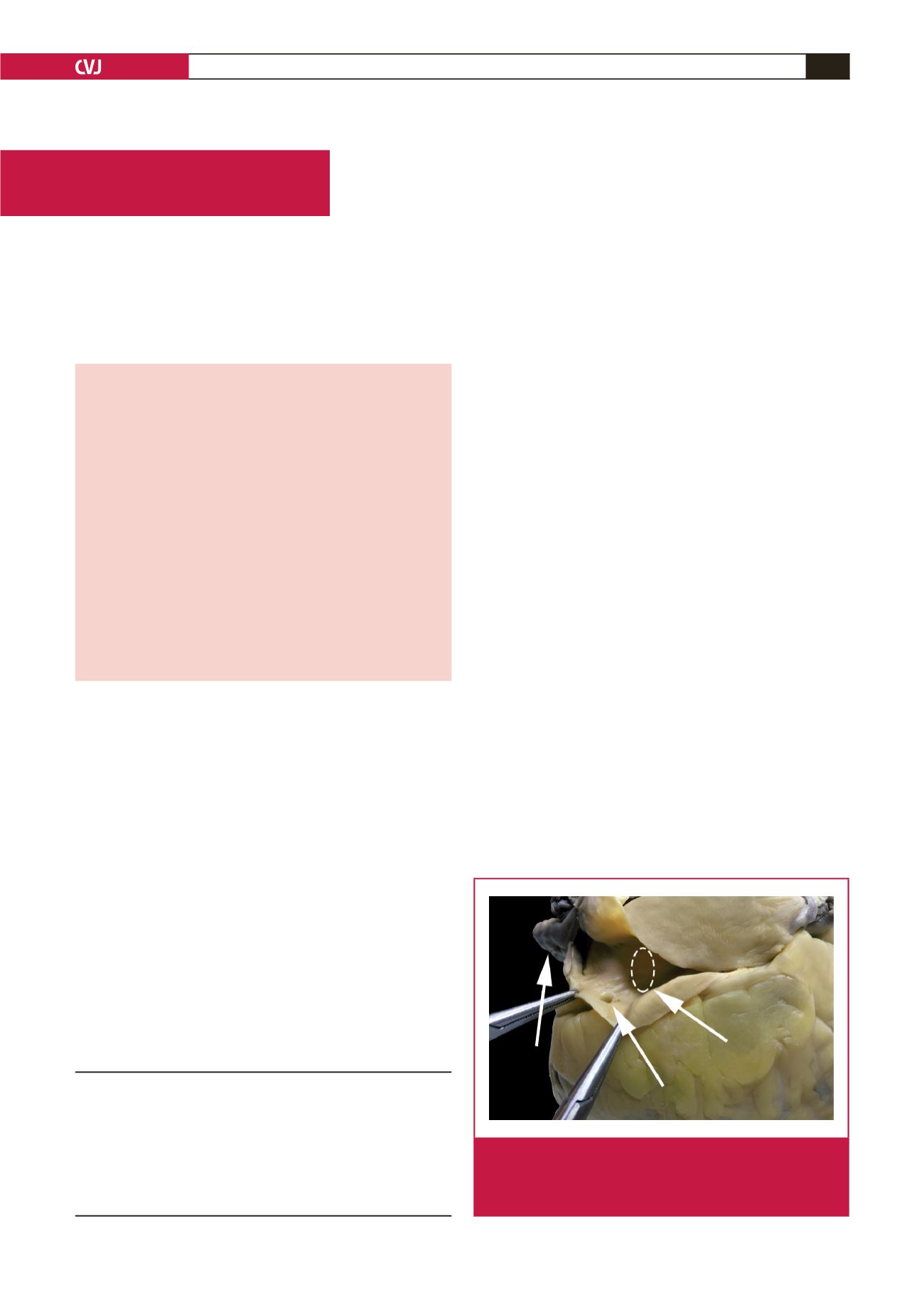
PLSVC
GCV
CS
Fig. 1.
The persistent left superior vena cava drains into the
coronary sinus in this heart specimen. CS, coronary
sinus; GCV, great cardiac vein; PLSVC, persistent left
superior vena cava.