
















 75 / 80
75 / 80

CARDIOVASCULAR JOURNAL OF AFRICA • Volume 28, No 3, May/June 2017
AFRICA
e5
A rare cause of early repolarisation in an adolescent boy
with chest pain: myocardial bridging
Murat Deveci, Kadir Babao
ğ
lu, Özlem Kayabey
Abstract
Early repolarisation is a common electrocardiographic (ECG)
finding characterised by J-point and ST segment elevation
≥
0.1 mV in two or more adjacent leads. The ECG pattern
of early repolarisation is relatively common in asymptomatic
subjects. Early repolarisation pattern may be seen in second-
ary conditions such as hypothermia, autonomic nervous
system disturbances, cocaine abuse, hypercalcaemia and
myocardial ischaemia. We present a case of an adolescent
boy with chest pain and concurrent ST-segment elevation.
Early repolarisation pattern was observed in the inferior leads
of the ECG with increased troponin levels. He was shown
to have myocardial bridging of the left anterior descending
artery. The coronary anomaly was not associated with left
ventricular hypertrophy. He was asymptomatic and the ECG
changes normalised on the third day after admission. The
patient was restricted from strenuous exertion and metoprolol
was prescribed for prophylaxis.
Keywords:
myocardial bridging, early repolarisation, chest pain,
adolescent
Submitted 10/1/16, accepted 16/10/17
Cardiovasc J Afr
2017;
28
: e5–e7
www.cvja.co.zaDOI: 10.5830/CVJA-2016-088
Myocardial bridging is characterised by the systolic compression
of amajor coronary artery segment by the overlyingmyocardium.
Although early reports considered it as a benign condition, it is
currently known to be associated with myocardial ischaemia and
infarction.
1
Early repolarisation is defined as J-point and ST-segment
elevation
≥
0.1 mV in two or more contiguous leads. The
ECG pattern of early repolarisation was initially described
as a normal variant because of its occurrence in one to
13% of the general population. Athletes, particularly those
participating in competitive sport, have a higher prevalence of
early repolarisation. The judgment that early repolarisation
was a benign finding devoid of clinical significance changed as
studies determined an association between the presence of early
repolarisation and an increased risk for arrhythmic death.
2-4
We present a patient with chest pain who had ST-segment
elevation (STE) and increased troponin levels and was found
to have myocardial bridging. Early repolarisation pattern in the
inferior leads was thought to result from ischaemia caused by the
myocardial bridging, which adds uniqueness to the presentation.
Case report
A 17-year-old boy was admitted to the emergency department
with burning, exertional chest pain that persisted for two hours.
His past medical history was unremarkable. He was a football
player in the school team and trained regularly. The patient
was not taking any medication and denied the use of illicit
substances. No previous chest pain with or without exercise was
described.
His family history was unremarkable for hyper-
homocysteinaemia, familial hyperlipidaemia and sudden death.
Haemodynamic parameters and systemic examination on
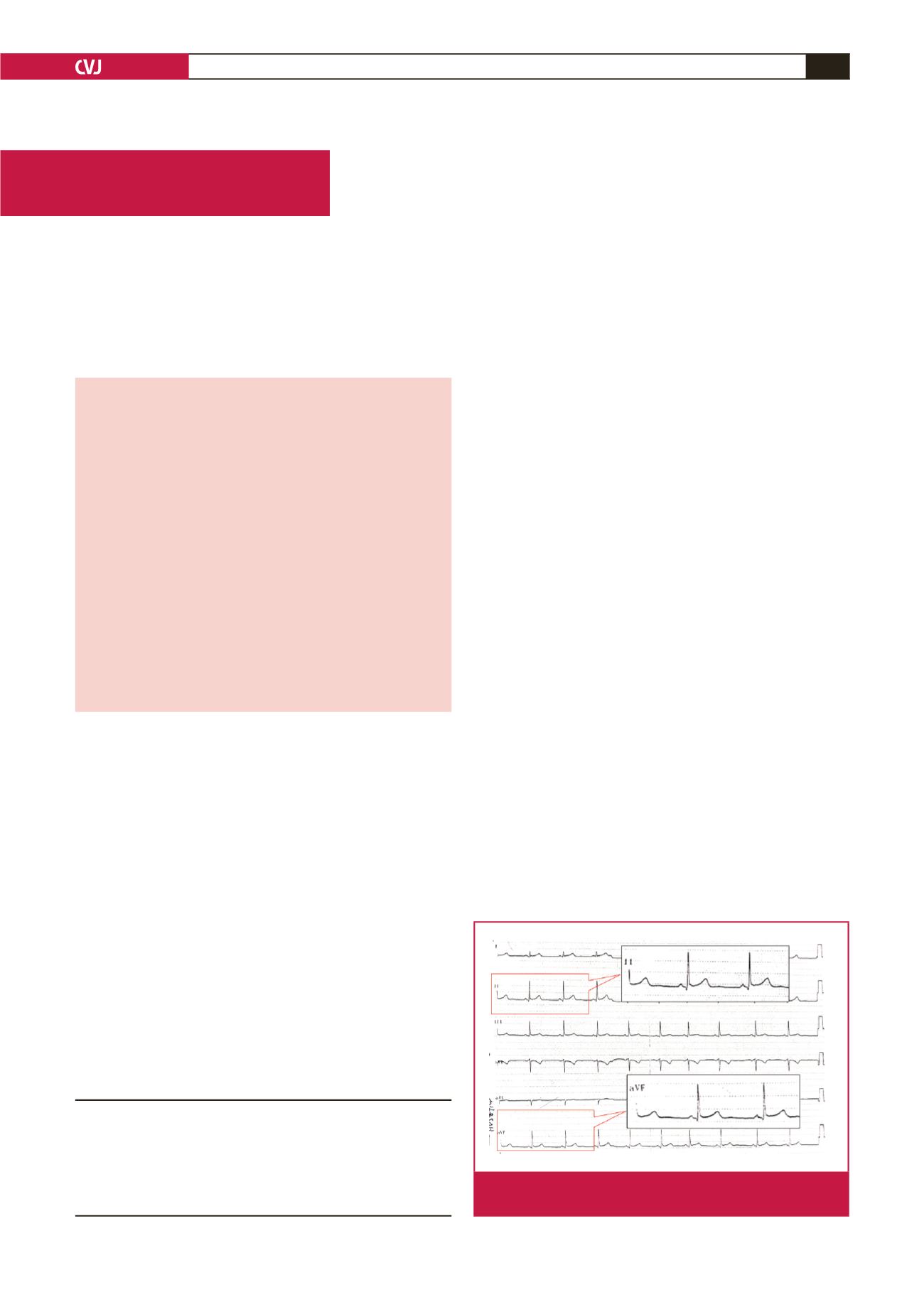
admission were negligible. The initial ECG showed normal sinus
rhythm with early repolarisation pattern in the inferior leads
(Fig. 1). Blood test values were all within the normal range,
except troponin. On hospital admission, his troponin level
was increased to 0.42 mg/ml and over two days at eight-hour
intervals, his troponin level was undulant (0.42,
<
0.01, 0.34,
Division of Paediatric Cardiology, Department of
Paediatrics, Kocaeli University School of Medicine,
Umuttepe-Kocaeli, Turkey
Murat Deveci, MD,
devemurat@gmail.comKadir Babao
ğ
lu, MD
Özlem Kayabey, MD
Case Report
Fig. 1.
ECG on admission shows early repolarisation pattern
in leads II, aVF.