
















 10 / 88
10 / 88

CARDIOVASCULAR JOURNAL OF AFRICA • Volume 28, No 4, July/August 2017
212
AFRICA
The method we used was to identify and select cases of
EMF from patients attending our echocardiography laboratory
using predefined features and definitions. All images relate to
advanced forms of EMF, which were available in the hospital
setting. We did not see mild or early forms of the disease and
speculate that population-based studies are more appropriate for
reporting these types of EMF.
4
As we recognised only 23 cases of EMF during the course of
eight years, we infer that the disease is rare in Sudan and that
only isolated cases are prevalent. Consequently, a study of this
nature will help improve the awareness of physicians to diagnose
this disease.
The basic diagnostic echocardiographic features are shown in
Figs 1 to 3. The images of apical and ventricularwall fibrosis together
with huge atria should alert the investigator to the possibility of
EMF. The presence of moderate-to-severe atrioventricular valve
regurgitation and obliterated ventricles should provide further
confirmation of the diagnosis (Fig. 1A, Fig. 2B, C).
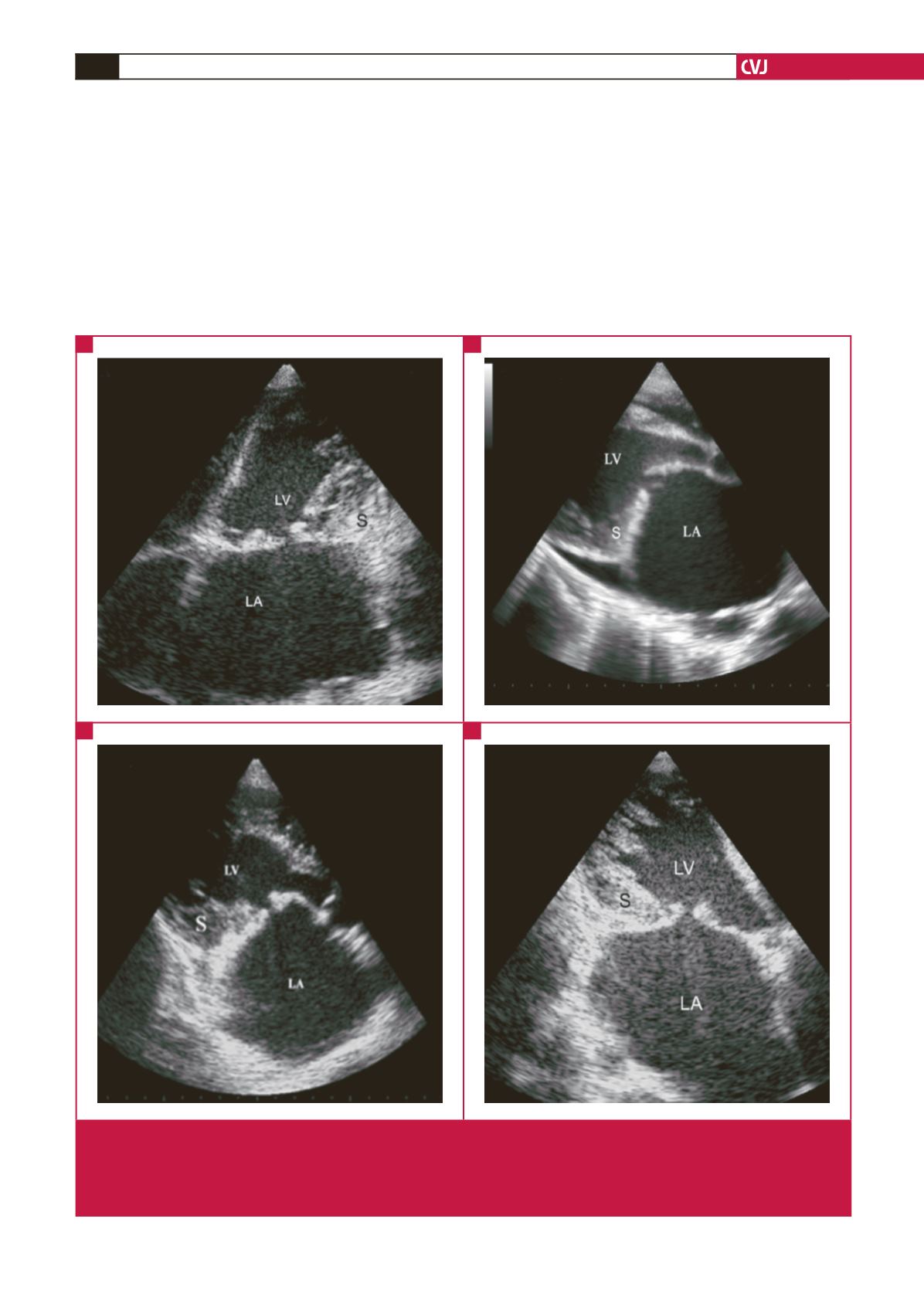
Fig. 5.
Endocardial fibrous shelf. A is PLAX, B is AP4, and C and D are modified APLX views from three different patients (B and
D from same patient), with left ventricular EMF showing thickened endocardium spreading over the recess between the
posterior papillary muscle and the posterior mitral valve leaflet, engulfing the leaflet and forming an immobile endocardial
fibrous shelf (S). The anterior mitral valve leaflet although moderately thickened, moves freely, while the whole mitral struc-
ture appears reduced to a single leaflet valve.
A
B
C
D