
















 32 / 74
32 / 74

CARDIOVASCULAR JOURNAL OF AFRICA • Volume 28, No 5, September/October 2017
306
AFRICA
ago, were followed up for a mean period of 5
±
2 years. None of
the patients had recurrence of CHD. One of our patients who had
CHD in the left ventricular posterior wall (Fig. 4) had re-operation
two years after cystectomy because of severe mitral insufficiency
and the mitral valve was repaired using an annuloplasty ring.
Discussion
Hydatid cyst is an important parasitic infection caused by
the larvae of the
Echinococcus granulosus
tapeworm. Some
carnivores (most often dogs) are the definitive hosts. Although
it is believed not to be a common health problem in developed
countries, the most common presentation of the disease is in
endemic areas such as Asia, the Middle East, the Mediterranean
region, South America, New Zealand and Australia.
1
It may be
seen in any organ or tissue in humans, but is most commonly
seen in the liver and lung. Cardiac involvement is rare and
comprises about 0.5 to 2% of all cases.
2
The involvement of CHDmay be either primary or secondary.
Primary involvement of the heart usually occurs via the coronary
circulation; the intestinal lymphatics, thoracic duct, vena cavae
and patent foramen ovale may be other pathways.
4
Secondary
involvement occurs from dissemination of the cyst from adjacent
organs, including the lungs, mediastinal structures or liver
through the diaphragm.
5
The most common involvement of CHD
includes the myocardium, mostly in the left ventricle (50–70%),
followed by the atria and free wall of the right ventricle (30%),
the pericardium (15–25%) and the interventricular septum
(5–15%).
6
In our series, the most common location of the CHD
was left sided (six patients, 50%). Five (41.7%) patients had CHD
in the right heart, whereas one patient (8.3%) had one in the
interventricular septum.
Until the late phase of the disease, patients usually do not
seek medical help, probably because it remains asymptomatic for
a long period of time. Presenting symptoms of CHD are variable
depending on the size, number and location of the cysts.
7
As the
cysts grow and reach reasonable sizes, patients may present with
chest pain, palpitations and dyspnoea. Only 10% of patients,
particularly those with large HCs have clinical manifestations.
Precordial pain is the most common symptom and is most often
vague and does not resemble angina pectoris.
8
When the cyst is located near the valvular apparatus, it may
stimulate valvular stenosis or cause valvular regurgitation.
9
In our series, one patient had severe mitral regurgitation after
resection of the HC located over the posterior wall of the left
ventricle, which may have been the cause for further mitral valve
repair. Although CHD may mimic any valvular pathology, or
pericardial or coronary artery disease of the heart, there are no
specific symptoms regarding the diagnosis of CHD.
Routine laboratory tests are not specific and may reveal
both normal and abnormal results. Blood count may show
eosinophilia, but it may also be completely normal. Serological
tests such as IHA and ELISA can assist in the diagnosis of HC
infection, but since they have a sensitivity of only 80%, false
negative results should be considered.
10
Usually the diagnosis starts with clinical suspicion of the
disease. Plain chest X-rays may give negative results in the early
phase of the disease. If theHChas a calcified outer layer or has led
to an increase in cardiothoracic index, or caused a deformation
over the borders of the heart, the X-ray may provide valuable
data, but accurate diagnosis is made by echocardiography, CT
or MRI studies. Sometimes the cyst may be found incidentally
from non-specific radiological or echocardiographic evaluations.
In detecting CHD, transthoracic echocardiography should be
the first choice, since it is non-invasive with a high sensitivity to
demonstrate the mass.
CT or MRI should also be used in order to demonstrate the
extent of the cyst and anatomical relationships prior to surgery.
CT is superior for observing intracystic gas, minute calcifications
and in anatomical mapping.
11
Cysts may be identified as uni- or
multilocular. Pathognomonic findings are the presence of a
Fig. 3.
Magnetic resonance image showing the cystic mass in
the interventricular septum (white arrow).
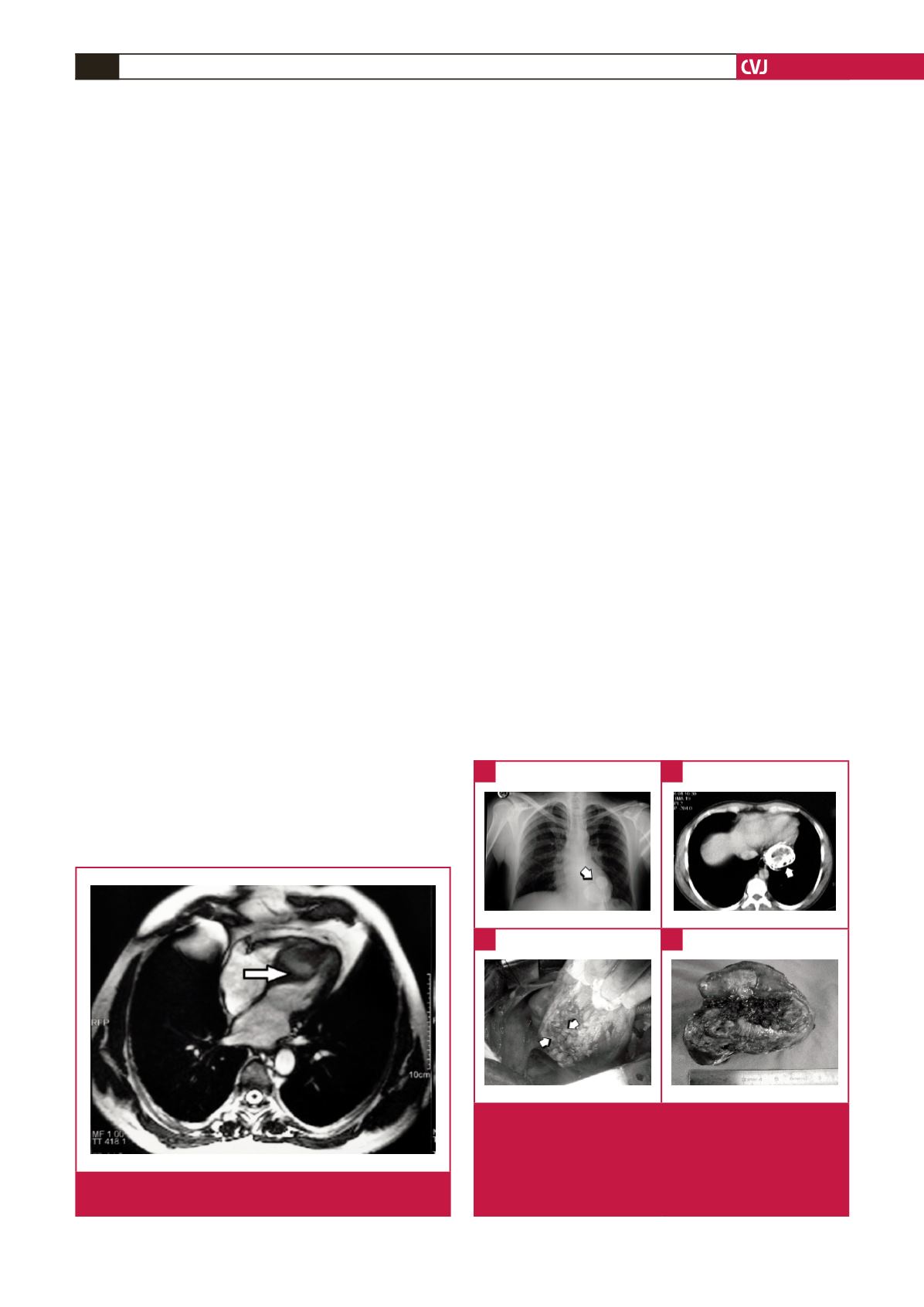
Fig. 4.
A. Plain chest X-ray showing the calcified outer layer
of the cardiac hydatid cyst. B. Eggshell appearance
of the cardiac hydatid cyst located on the posterior
left ventricular wall on computerised tomography. C,
D. Surgically closed defect after removal of the highly
calcified hydatid cyst.
A
C
B
D