CARDIOVASCULAR JOURNAL OF AFRICA • Vol 21, No 4, July/August 2010
226
AFRICA
Thereafter the patient was asymptomatic with no further
syncope attacks for a period of a year. Because of the asympto-
matic period, the patient stopped the metoprolol and paroxetine
without medical consultation in 2005.
Two weeks before admission to our hospital, the
episodes of syncope reappeared more intensely than before.
Electrocardiography on admission demonstrated non-torsade
de pointes ventricular tachycardia (Fig. 1). The regular ECG
after admission showed ventricular ectopic beats (Fig. 2A) and
supraventricular ectopic beats (Fig. 2B). Subsequent ambulatory
ECG monitoring (22 hours and 53 min) after hospitalisation
demonstrated a ventricular rate varying from 101 to 40 beats per
minute and frequent polymorphic premature ventricular contrac-
tions with 416 episodes per hour.
A comprehensive biochemical evaluation, which included
a coagulation profile, liver and kidney functions, electrolytes,
glucose, auto-antibodies, thyroid hormone levels and thyroid
antibodies, and antibodies to Coxsackie virus, were all within
normal limits. Resting echocardiography showed normal cardiac
structure and function, mild mitral regurgitation, the left atrial
dimension was 38 mm (25–40 mm), interventricular septum
(IVS) was 11 mm (6–11 mm), left ventricular dimensions (LVIDd
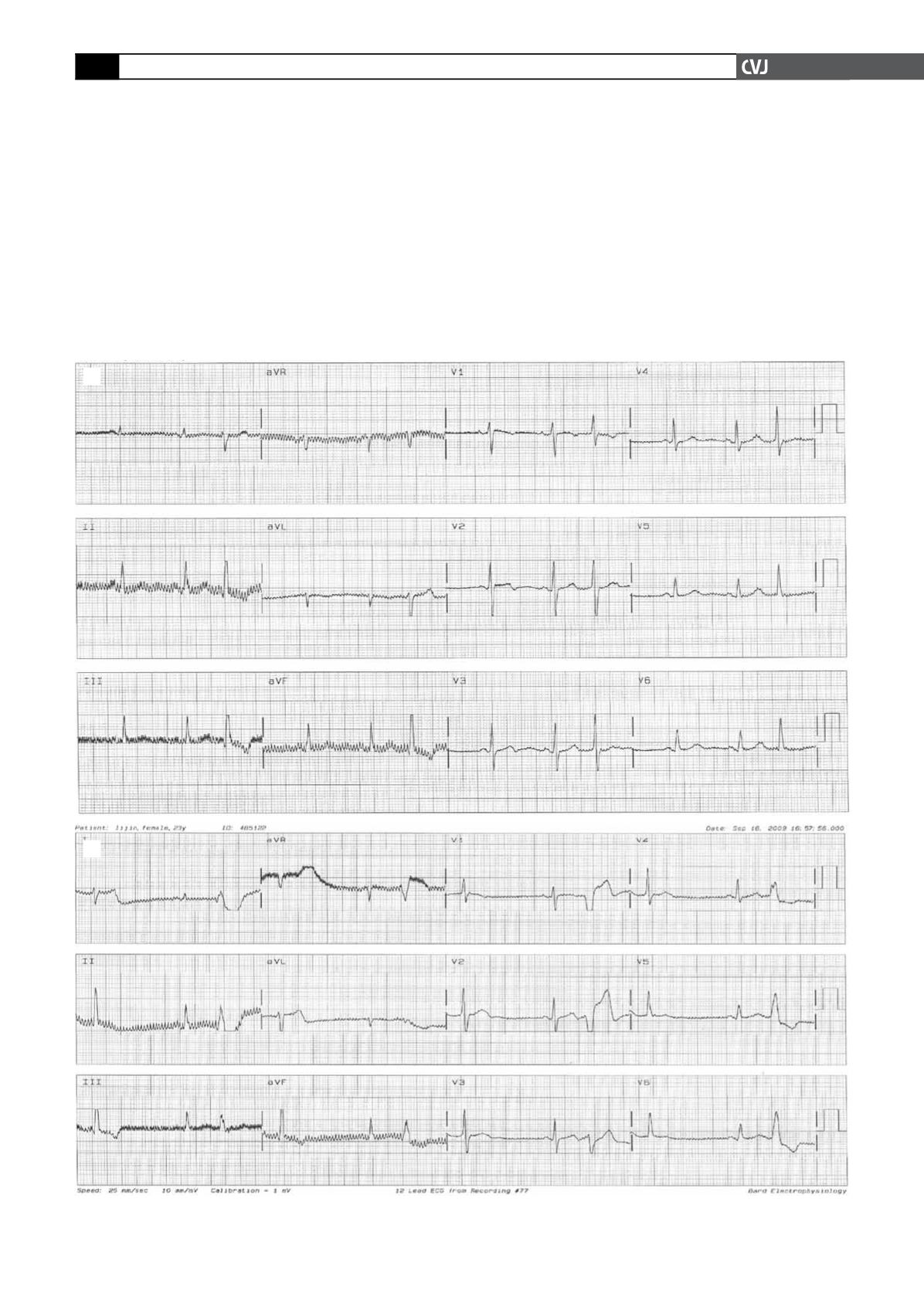
Fig. 2. Regular ECG after admission. A: ventricular beats, B: supraventricular ectopic beats.
A
B


