CARDIOVASCULAR JOURNAL OF AFRICA • Vol 22, No 5, September/October 2011
264
AFRICA
hypertensive group. In the whole group, 62.3% of participants
had normal BP control. In the hypertensives receiving therapy,
only 35.9% had normal BP control and hence should have
received additional antihypertensive drug therapy; 42.5% of
patients with untreated hypertension and 23.9% of patients with
treated hypertension had moderate to severe increases in BP.
Table 3 shows the classes of agents and number of classes of
antihypertensive agents used to treat BP in the controlled and
uncontrolled hypertensives. Importantly, the majority of patients
were receiving diuretic monotherapy. No differences were noted
in the classes of agents and number of classes of antihypertensive
agents employed in the hypertensives controlled to target BP
compared to those not at target BP.
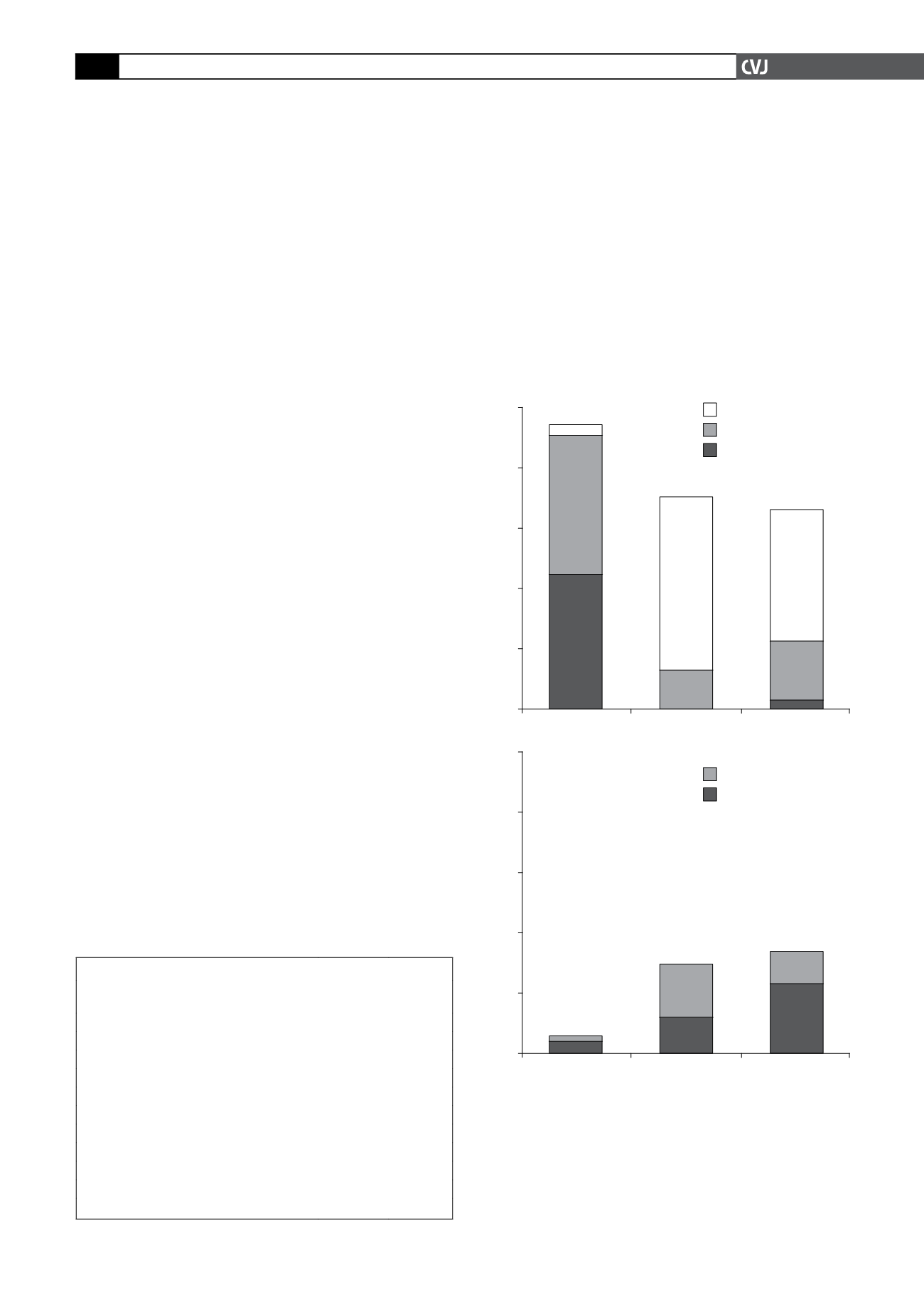
Fig. 1 shows the distribution of cardiovascular risk profiles
in normotensive participants, hypertensive patients not receiving
therapy, and hypertensive patients receiving therapy, based on
the SAHS and the ESH/ESC guidelines. Importantly, in hyper-
tensives not receiving therapy, 29.6% of participants had either
high (~12%) or very high (~18%) added cardiovascular risk.
Therefore, based on the SAHS and ESH/ESC guidelines, in the
community at large, 6.7% of participants had untreated hyperten-
sion together with a high or very high added cardiovascular risk.
With regard to the risk profiles of participants, determined
from the WHO/ISH guidelines for low- and middle-income
countries, 0.2% of normotensives, 11.2% of untreated hyperten-
sives and 12.8% of treated hypertensives had a
>
30% chance
of a cardiovascular event in 10 years. These proportions were
similar to the proportions noted with a very high added risk, as
defined by the SAHS/ESH/ESC guidelines (Fig. 1).
Table 4 shows the factors contributing to cardiovascular
risk, as defined by the SAHS/ESH/ESC guidelines in untreated
hypertensives. Importantly, while no participants in the lower-
risk category had severe hypertension, DM or cardiovascular
disease, of the participants with a high or very high added risk,
52.2% had severe hypertension (36/69 participants), 33.3% had
DM (23/69 participants), and 8.7% had an associated cardio-
vascular condition (6/69). None of the participants with DM
had severe hypertension. An increased prevalence of ‘risk’ age
(men
>
55 years and women
>
65 years), dyslipidaemia, and an
increased waist circumference was also noted in the high or very
high added risk category.
In contrast to the factors that characterised a higher versus
lower cardiovascular risk in participants, as defined by the
SAHS/ESH/ESC guidelines, where no participants in the lower-
risk categories had severe hypertension or DM, according to
the WHO/ISH guidelines, 9.2 and 7.3% of those with a
<
30%
chance of a cardiovascular event in 10 years had severe hyper-
tension or DM, respectively. Moreover, when defining risk
according to the WHO/ISH guidelines, no differences in either
the proportion of participants with general or central obesity, and
no differences in mean BMI or waist circumference were noted
between those participants with a
<
30% or
>
30% chance of a
cardiovascular event in 10 years (data not shown).
Discussion
The main findings of the present study are as follows. In an
urban, developing community of African ancestry, 22.6% of
TABLE 3. DRUGTHERAPY IN TREATED HYPERTENSIVES
Uncontrolled
BP (
n
=
155)
Controlled
BP (
n
=
87)
% monotherapy
71.0
67.8
% dual therapy
18.0
24.1
% more than 3 agents
11.0
8.1
% diuretic monotherapy
62.6
58.6
% diuretics with other agents
28.4
31.0
Angiotensin-converting enzyme inhibitors (%)
17.4
18.4
Angiotensin receptor blockers (%)
0.7
0
Calcium channel blockers (%)
12.3
14.9
β
-adrenergic receptor blockers (%)
2.6
1.2
Others (%)
19.4
17.2
BP: blood pressure.
Fig. 1. Cardiovascular risk profiles in normotensive,
untreated hypertensive and treated hypertensive partici-
pants in an urban, developing community of African
ancestry. The levels of risk are defined according to
current Southern African Hypertension Society
27
and
European Society of Hypertension/European Society of
Cardiology
16
guidelines. High and very high added risk
are risk scores that require the initiation of antihyperten-
sive medication. HT: hypertension; NT: normotension.
100
80
60
40
20
0
NT
Untreated HT
Treated HT
Frequency (%)
3
46
45
57
13
43
20
3
Moderate added risk
Low added risk
Average added risk
100
80
60
40
20
0
NT
Untreated HT
Treated HT
Frequency (%)
2
4
18
12
11
23
Very high added risk
High added risk


