CARDIOVASCULAR JOURNAL OF AFRICA • Vol 22, No 5, September/October 2011
AFRICA
275
divide the right ventricular cavity into a proximal high-pressure
chamber and a low-pressure chamber distal to the hypertrophied
muscle bands.
1-3
In the majority of patients, VSD or pulmonary
valve stenosis is also present, although rarely, it can occur as an
isolated disorder.
2
Anatomically, the anomalous hypertrophied muscle bundles
constitute a pyramidal mass of muscle that runs between the
ventricular septum inferior to the insertion of the septal leaflet
of the tricuspid valve to the anterior wall of the right ventricle.
1,3
There are usually two bundles: the ventral bundle, which attaches
to the wall of the right ventricle adjacent to the septum, and the
dorsal bundle, which is the largest and attaches to the base of the
anterior papillary muscle. The right ventricular cavity is divided
into a proximal portion, which consists of the sinus portion of
the right ventricle, and a distal portion, which consists of the
infundibulum.
1
There are several subtypes of DCRV.
4
These include: anoma-
lous septoparietal band, anomalous apical shelf, hypertrophy
of apical trabeculations, anomalous apical shelf with Ebstein
malformation, and sequestration of the outlet portion of the
ventricle from a circumferential muscular diaphragm in patients
with tetralogy of Fallot (TOF). Double-chambered right ventri-
cle, the most common form, is noted by the presence of anoma-
lous muscle bundles that divide the right ventricle into two
chambers. However, no uniformity is observed in the position of
these anomalous muscle bundles or in the manner in which the
right ventricle is divided.
4
In TOF, the obstruction involves the infundibular area but the
anomalous bundle in a double-chambered right ventricle crosses
the right ventricular cavity to lie proximal to the infundibulum.
The orientation of these muscle bands differs from those of the
moderator bands. Although both types of muscle bundles attach
to the anterior wall of the right ventricle, the moderator bands
lie towards the septum and do not ordinarily obstruct the cavity,
whereas in the anomalous muscle bundles, the septal branches
are near the base of the tricuspid valve ring.
The origin of the anomalous muscle bands is unknown.
1,5
It is believed that they may be due to localised growth of the
trabeculated myocardium early in development. It has also been
suggested that the right ventricular subdivision and obstruction
in this malformation represent an arrested incorporation of the
primitive bulbus cordis into the right ventricular body.
1,5
The irregular expansion of the bulboventricular junction
would therefore result in incomplete fusion of the bulbar and
endocardial cushion elements that commonly close the supe-
rior portion of the ventricular septum. This would explain the
frequent association of a VSD with this malformation.
3,6
The
VSD is most frequently found in the peri-membranous septum
and sometimes in the sub-arterial location.
Associated defects are present in approximately 80 to 90%
of patients. A VSD that involves the membranous septum is the
most common defect described. A VSD may communicate with
either the proximal or distal chamber, leading to a greater shunt
in the latter situation. Development of a right ventricular outflow
tract obstruction occurs in 3 to 7% of patients with membranous
VSDs within the first years of life. The mechanism responsible
for acquired right ventricular obstruction may be progressive
hypertrophy and obstruction from anomalous right ventricular
muscle bundles.
1,3
A well-known relationship is described among patients with
right ventricular outflow tract obstruction, membranous VSD,
and sub-aortic stenosis. Vogel
et al
. described 36 patients with
membranous VSD and a double-chambered right ventricle, 88%
of whom had echocardiographic evidence of sub-aortic steno-
sis with evidence of progressive left ventricular outflow tract
obstruction.
7
Progression of sub-aortic stenosis may occur before
or after VSD closure and/or the muscle bundles are resected.
3
The next most common associated lesion is pulmonary valve
stenosis. Various other associations have been reported, includ-
ing a double-outlet right ventricle, tetralogy of Fallot, anomalous
pulmonary venous drainage, complete or corrected transposition
of the great arteries, pulmonary atresia with intact ventricular
septum, and Ebstein anomaly. Double-chambered right ventri-
cle has also been reported in patients with Down and Noonan
syndromes, although differentiation from hypertrophic cardio-
myopathy in the latter group is not straightforward.
2,3
A double-chambered right ventricle is relatively rare as an
isolated anomaly; a large paediatric centre typically diagnoses
fewer than 10 cases per year. The lesion makes up approximately
0.5 to 2% of the coronary heart disease cases and occurs in as
many as 10% of patients with VSD.
5
Male-to-female ratio is
2:1. No inheritance pattern has been described. No risk factors
for developing the disease have been encountered. Sporadic
cases have been described in patients with Down and Noonan
syndromes.
3
Presentation can be as early as the newborn period, however
mean age at diagnosis is in early childhood. Both foetal and
adult cases have been reported. Often non-obstructive anoma-
lous muscle bundles in infancy become obstructive later. Most
patients with DCRV initially present with no symptoms. The
most common reason for referral is the detection of a murmur.
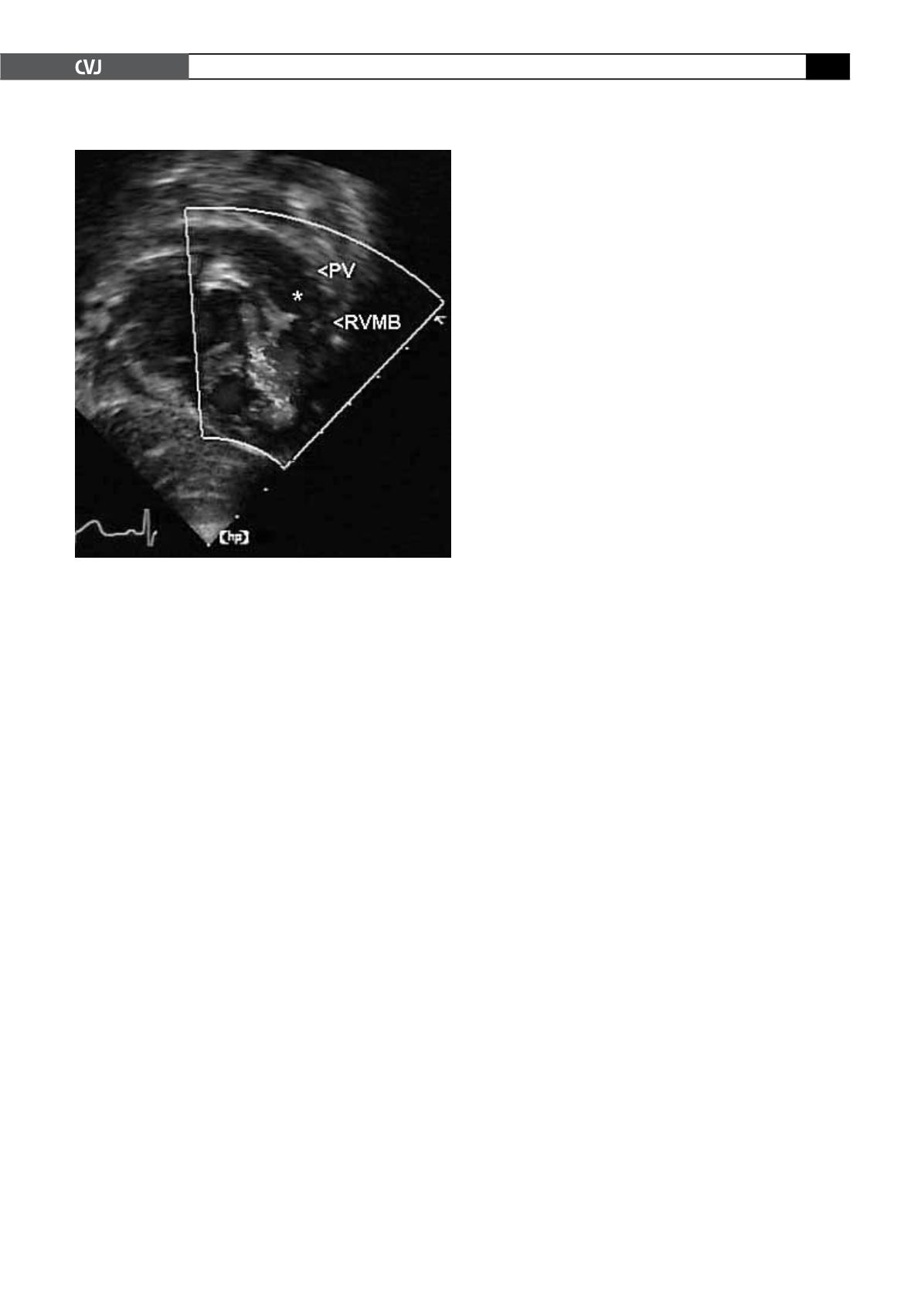
Fig. 1. Colour Doppler echocardiography shows signifi-
cant muscle bundles in the right ventricular outflow tract
with a small peri-membranous ventricular septal defect
and a severe double-chambered right ventricle with
right ventricular outlet tract gradient of 104 mmHg. PV
=
pulmonary valve, RVMB
=
right ventricle muscle band.


