CARDIOVASCULAR JOURNAL OF AFRICA • Vol 23, No 10, November 2012
AFRICA
555
non-familial ones. Although the disease has been associated
with enteroviral and adenoviral myocarditis, it is not considered
to be primarily caused by myocarditis. Lately it has been shown
that the disease is not confined to the right ventricle as the name
suggests, because the left ventricle may be affected in up to 75%
of the patients.
12
Other genetic disorders of the myocardium
Familial and non-familial cases have been described in patients
with the recently discovered myocardial disorder known as
left ventricular non-compaction (LV non-compaction).
12
Characteristic morphological changes of this disease are often
found in the left ventricle of those with the disease. There
are no reports of LV non-compaction from Africa, possibly
because African cardiologists are not yet familiar with its
echocardiographic changes.
Genetic disorders of the electrical system of the myocardium
with or without morphological changes have also been described.
They include Lenegre disease,
17
a progressive disease of the
conduction system of the heart and the ion channelopathies.
Among the ion channelopathies are the long-QT syndrome,
Brugada syndrome, catecholaminergic polymorphic ventricular
tachycardia, short-QT syndrome and idiopathic ventricular
fibrillation, all of which can cause sudden death. Lenegre disease
and the long-QT syndromes are well-known entities in clinical
practice in Africa although long-QT is only associated in Africa
with metabolic problems, particularly potassium deficiency
following prolonged treatment with diuretics. It is however
interesting to note the recent report from South Africa,
24
which
concluded that the genetic forms of long-QT syndrome (LQTS)
occurred most commonly among the white Caucasian population
of South Africa, with fewer cases from those of mixed ancestry
and none from those of black African descent.
2
The other ion
channelopathies have not been reported from Africa, probably
because of lack of sophisticated cardiac electrophysiological
studies and a dearth of well-trained personnel required to make
the diagnosis.
Dilated cardiomyopathy
Next to hypertension, this is the commonest cause of heart
failure in black Africans.
1,2
In some communities in Africa,
DCM is the commonest cause of heart failure. Before the advent
of echocardiography, the diagnosis was made on the basis of
clinical presentation, chest X-ray, ECG, and sometimes in the
large teaching hospitals, cardiac catheterisation and angiography.
Echocardiography has made the diagnosis easier and is presently
the preferred investigation for making a diagnosis.
Affected patients often presented in congestive cardiac failure
with functional mitral and tricuspid regurgitation due tomyocardial
failure, the cause of which was not apparent. ECG changes were
variable. Some had low-voltage complexes while others presented
with left ventricular hypertrophy. Abnormal intraventricular
conduction defects were common, especially left bundle branch
block. Chest X-ray usually showed cardiomegaly with failure,
while angiography confirmed a dilated left ventricle with poor
myocardial contraction and functional mitral regurgitation.
DCM is widely regarded as an end-stage myocardial disease
from a wide variety of adverse factors. The most common of
these insults are briefly considered below.
Hypertension
For a long time, several workers in Africa had suspected that
many patients who were labelled as having DCM were really
hypertensives. And there had been several debates at world
conferences where this assertion was actively advanced by
many workers. Mokhobo,
25
from South Africa advised caution
in making a diagnosis of cardiomyopathy since ‘cardiomyopathy
and hypertension are both common in black patients and
confusion may arise between them’. Lowenthal,
24
also from South
Africa wrote as follows: ‘these cases are regarded as evidence
in favour of the hypothesis that many cases of cryptogenic
heart disease (cardiomyopathy, congestive cardiomyopathy,
idiopathic cardiomegaly) are in fact hypertensives presenting
with normotensive cardiac failure’.
From Nigeria, Brockington,
26
after extensive studies, came
to the conclusion that hypertension and what he called heart
muscle disease at the time were similar and that the latter was
‘
the late stage of untreated chronic hypertensive heart failure’.
Brockington’s view was supported by Celia Oakley at a debate
during a conference on cardiomyopathies held in London in 1971
but John Goodwin at the same conference disagreed, asserting
that hypertensive heart disease was structurally different from
heart muscle disease.
The contentious problem in the past had always been the
presenting blood pressure. Some patients had a normal blood
pressure at presentation but in others the blood pressure was
mildly raised, although out of proportion with the degree of
the patient’s heart failure. Very often, the hypertension was
transient, the blood pressure becoming normal with treatment of
the heart failure and staying normal without sustained treatment
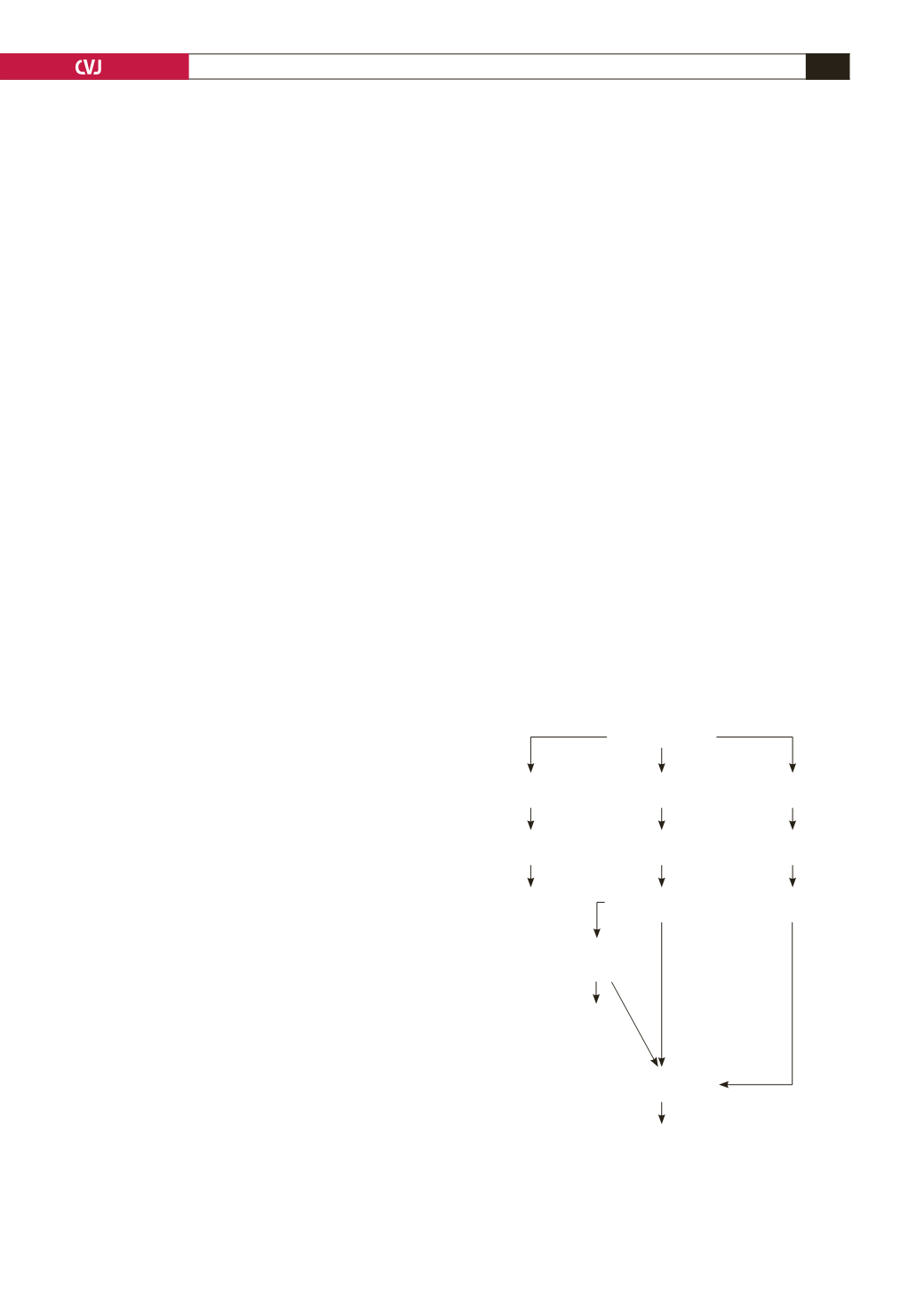
Fig. 3. The consequences of myocardial fibrosis on the
heart of patients with arterial hypertension, modified
from Diez
et al
.
Nature Clin Pract Cardiovasc Med
2005;
2(4): 209–216.
Fibrosis
Ventricular
arrhythmias
Ischaemia
Diastolic
dysfunction
Heart failure
Ventricular
arrhythmias
Sudden death
Systolic
dysfunction
Architectural
disarray
Extravascular
compression
Increased
myocardial stiffness
Decreased LV
distensibility
Compromised
LV filling
Myocardial fibre
necrosis with
reparative fibrosis
Interstitial
Perivascular


