CARDIOVASCULAR JOURNAL OF AFRICA • Vol 23, No 10, November 2012
556
AFRICA
with diuretics or hypotensive agents. Some investigators had
referred to this phenomenon as ‘reactive hypertension’ or ‘Sahli’s
Hochdruckstauung’
27
because it was thought to be due to intense
peripheral vasoconstriction, which occurred in heart failure.
Studies from Nigeria in the seventies have however shown
that what was called heart muscle disease in the past was
not caused by a single disease process.
28-33
Over 75% of
patients were hypertensives whose hearts had become damaged
over time because of poor or lack of control of high blood
pressure.
34
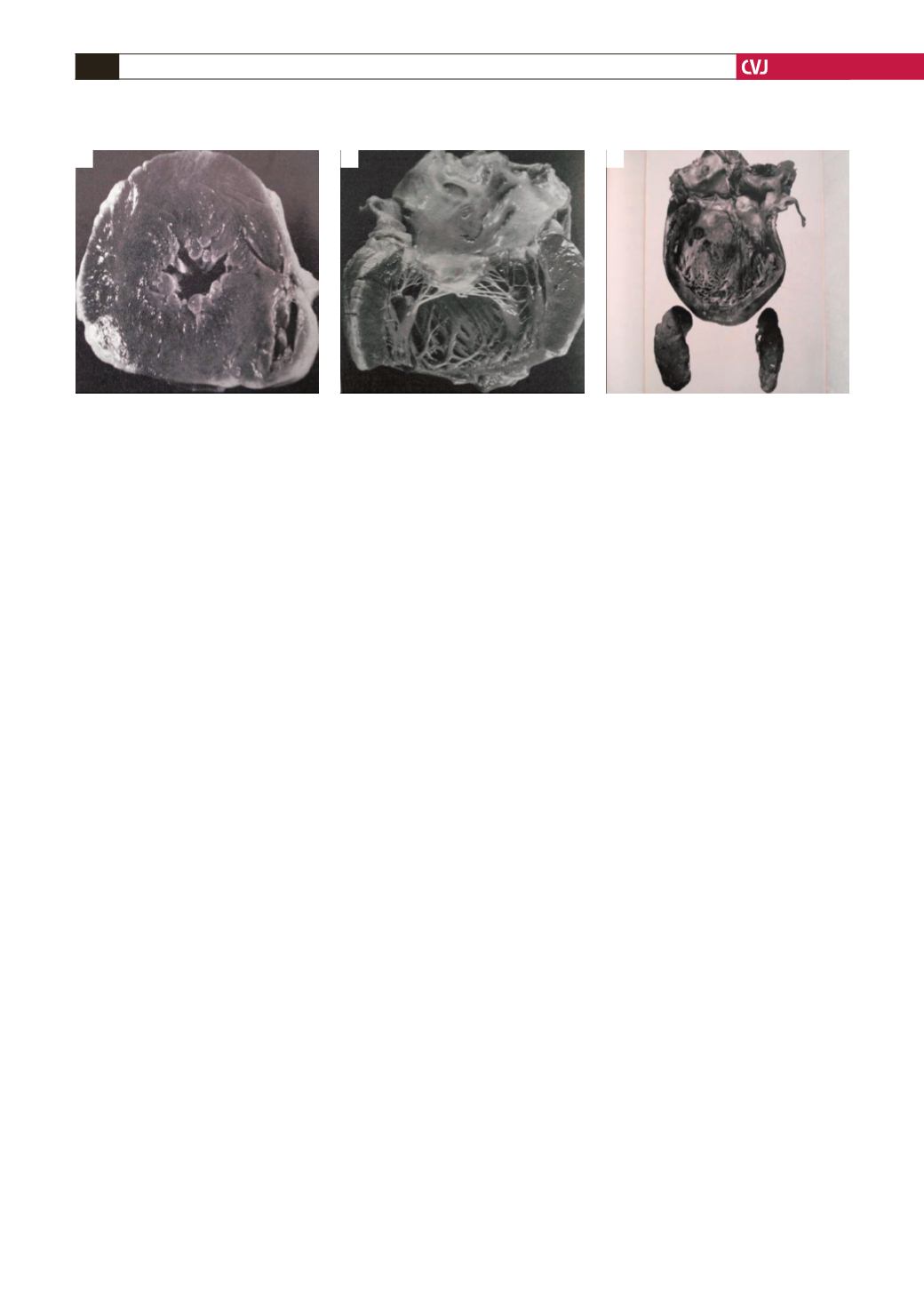
Progression from a hypertrophied heart (concentric
or asymmetric) in Nigerian hypertensives to the stage of flabby
heart has been discussed in an earlier publication (Figs 3, 4).
34
Alcohol
Early reports from Nigeria showed that alcohol consumption
played a significant part in the genesis of myocardial damage
of patients diagnosed with cardiomyopathies. The authors also
suggested that excessive consumption contributed to the heart
failure of some of their hypertensives.
29,35
This is in agreement
with Rees
et al
.
36
who in 1974 suggested from Nairobi that some
of their patients with cardiomyopathies were suffering from
the combined effects of excessive alcohol consumption and
hypertension, and this combination led to congestive cardiac
failure.
Some of the patients studied inNigeria had thiamine deficiency
and these were linked with protein malnutrition and excess
consumption of alcohol. All but one had low-output cardiac
failure and they did not respond to thiamine administration.
30
By contrast, high-output and low-output cardiac failure caused
by thiamine deficiency was shown to have equal prevalence in
South African alcoholics.
27
Generally, it is now estimated that alcohol is a contributory
factor in a significant number (up to 45%) of patients with heart
failure of unknown cause in Africa,
27
and alcohol also contributes
to the heart failure of a significant number of hypertensives.
Myocarditis
Studies in the seventies also showed that myocarditis was the
cause of a significant number of patients diagnosed at the
time as heart muscle disease of unknown cause, especially
among young people below the age of 30 years. At that time,
it was only possible to investigate the role of Coxsackie B
virus and
Toxoplasma gondii
in the patients studied, but higher
antibody levels were found in the patients compared with control
subjects. About 45% of the patients eventually turned out to be
hypertensive, implying that myocarditis was playing some part in
the genesis of their myocardial damage.
28-30,32
A few cases of acute myocarditis caused by Coxsackie B
3
virus and
Toxoplasma gondii
were documented during the four
years the patients were followed up. Sub-clinical infection by
Toxoplasma gondii
is common in Nigeria and several studies
have found that virtually everyone living in this community has
seroconverted to the organism.
32,33
Since then, several studies have confirmed the role of
myocarditis in the genesis of myocardial failure all over the
world and many more organisms [viruses including the human
immunodeficiency virus (HIV), bacteria including mycobacteria,
parasites such as
Trypanosoma, Toxoplasma gondii
and
Schistostoma
]
have been identified as culprits.
2
In Africa, many
patients with myocardial failure and a positive HIV test have
been shown to have not only viral myocarditis (HIV, Epstein-
Barr virus, cytomegalovirus, parvovirus, adenovirus and human
simplex virus) but also infections from other organisms such as
toxoplasmosis and cryptococcus.
Endomyocardial biopsies and detection of viral genomes
have been crucial in the identification of these agents in
the myocardium of the patient.
37,38
In an excellent study by
Shaboodien,
39
a prevalence of 100% infectivity (enterovirus,
Epstein-Barr virus, parvovirus, human simplex virus and
adenovirus) was found in the hearts of the patients with
‘
idiopathic dilated cardiomyopathy’ she biopsied. Unfortunately
these advanced techniques are not widely available in Africa
outside South Africa.
The role of excessive immune activation in the pathogenesis
of the disease has also been studied in Africa. A study found that
HLA-DR1 and HLA-DRw10 were commoner in patients with
DCM.
40
Elevated plasma levels of inflammatory cytokine tumour
necrosis factor (TNF)-
α
,
C-reactive protein and a plasma marker
of apoptosis have also been found in DCM patients,
41-43
and
those with peripartum cardiomyopathy.
44
Leucocyte cytokines
were also found to be elevated in these patients. In those with
peripartum cardiomyopathy, the level of Fas/Apo-1 was also
elevated.
These findings had led to studies on the immunomodulatory
effect of pentoxifylline in the management of the DCM patients,
Fig. 4. Representation of progression of the left ventricle in hypertensive patients, from concentric hypertrophy with a
small cavity, to concentric hypertrophy with a large cavity, to a destroyed myocardium unable to sustain a high blood
pressure.
A
B
C


