CARDIOVASCULAR JOURNAL OF AFRICA • Vol 23, No 10, November 2012
AFRICA
553
ischaemic heart disease remains low, while that of rheumatic
heart disease has decreased considerably.
3
We are primarily concerned with myocardial diseases and
endomyocardial fibrosis in this discourse. We performed
a systematic search of Pubmed for published data on
cardiomyopathies in sub-Saharan Africa from January 1960 to
December 2009. This was supplemented with parallel searches
of references of identified journals, as well as a search of specific
data sets such as African Index Medicus, African Journals Online
(
AJOL) and the World Bank database. The search strategy
was Africa or sub-Saharan Africa and cardiomyopathy, dilated
cardiomyopathy, endomyocardial fibrosis, and peripartum
cardiomyopathy.
Prior to 1980 there were several descriptions from many
geographical areas of the world but mainly from Africa of
obscure forms of heart disease that primarily affected the
heart muscle. These descriptions were published under several
names such as idiopathic cardiomegaly,
4
nutritional heart
disease,
5
cardiovascular collagenosis with parietal endocardial
thrombosis,
6
and cardiomyopathy.
7
The common features of
these descriptions were that affected patients presented in
congestive cardiac failure with cardiomegaly, the cause of which
was not readily apparent. The disease was particularly common
in the tropical and sub-tropical countries of the world where it
constituted one of the major clinical and health problems.
8
Similarly, there were several descriptions from many parts
of the world, of another group of myocardial diseases that
was characterised by inappropriate massive hypertrophy of the
cardiac muscle (HCM). It was first described by Teare in 1958.
9
Prior to 1980, it appeared to have a worldwide distribution
although initial reports suggested that it was rare in black people.
The reason for this might have been due to a high prevalence
of hypertensive heart disease, which interfered with the correct
diagnosis of the disease.
10
HCM too had been described in the
past under several names, including idiopathic hypertrophic
sub-aortic stenosis, muscular sub-aortic stenosis, obstructive
cardiomyopathy and asymmetrical hypertrophy.
11
Thirdly, there were before 1980 several descriptions of
another group of myocardial disorders of unknown origin,
which was characterised by fibrosis of the endomyocardium,
particularly the inflow tract, apex and part of the outflow
tract of either or both ventricles. The mitral/tricuspid valve
apparatus, depending on which ventricular chamber was affected
was commonly enmeshed in fibrous tissue, which very often
involved the posterior valve leaflet. The anterior valve leaflet was
rarely involved. It was called endomyocardial fibrosis (EMF) in
those tropical countries that first reported it.
12
Prior to the description of the tropical forms of EMF, there
were also reports of a similar disease that was characterised
by the presence of hypereosinophilia. It was first described
by Löffler in 1936,
13
and was known as Löffler’s endocarditis
parietalis fibroplastica. This disease was initially believed to
be confined to only the temperate zones of the world and was
considered to be a separate illness from the tropical forms of
EMF. However several reports have now confirmed its presence
in Africa and other countries of the world where the tropical
forms of EMF is prevalent.
14
Some have even suggested that it is
the early form of tropical EMF (Fig. 2).
14
Classification of the cardiomyopathies
Because of the initial confusion arising from the names given to
all these diseases, the inadequacy of previous classifications,
15
and to ensure unanimity in their descriptions, a task force was
set up by the World Health Organisation and the International
Society and Federation of Cardiology (WHO/ISFC) to harmonise
the features of the diseases, adopt uniform names for them, and
design an acceptable classification. The report of the task force
was published in 1980,
11
while the full description of each
disease was published by the WHO as a report of an expert
committee in 1984.
10
At the 1980 meeting, it was agreed to adopt the name
‘
cardiomyopathy’ for all diseases of the heart muscle of unknown
cause. For a disease to qualify as a cardiomyopathy therefore,
the patient must have been extensively investigated and no cause
found for the malady. Diseases whose causes were known were
simply identified by their causative factors, such as alcohol heart
disease, myocarditis or viral heart disease. Such diseases were
grouped under a separate heading called ‘specific heart muscle
diseases’ which was defined as ‘heart muscle diseases of known
cause or associated with disorders of other systems’.
Since it was considered inappropriate to slot well-known
disorders of the myocardium caused by systemic or pulmonary
hypertension, coronary artery disease and congenital heart
diseases under this group, they were excluded from the
classification. It was felt that all diseases of the myocardium
would have had to be listed under specific heart muscle diseases
if this was not done. In summary, cardiomyopathy was regarded
as a disease of exclusion.
The meeting further agreed to group the cardiomyopathies into
three types. The first two were named to highlight the changes
in their structures (hypertrophic and dilated) while the third,
unfortunately, in our view, was named to reflect its restrictive
haemodynamic features (restrictive). This classification was
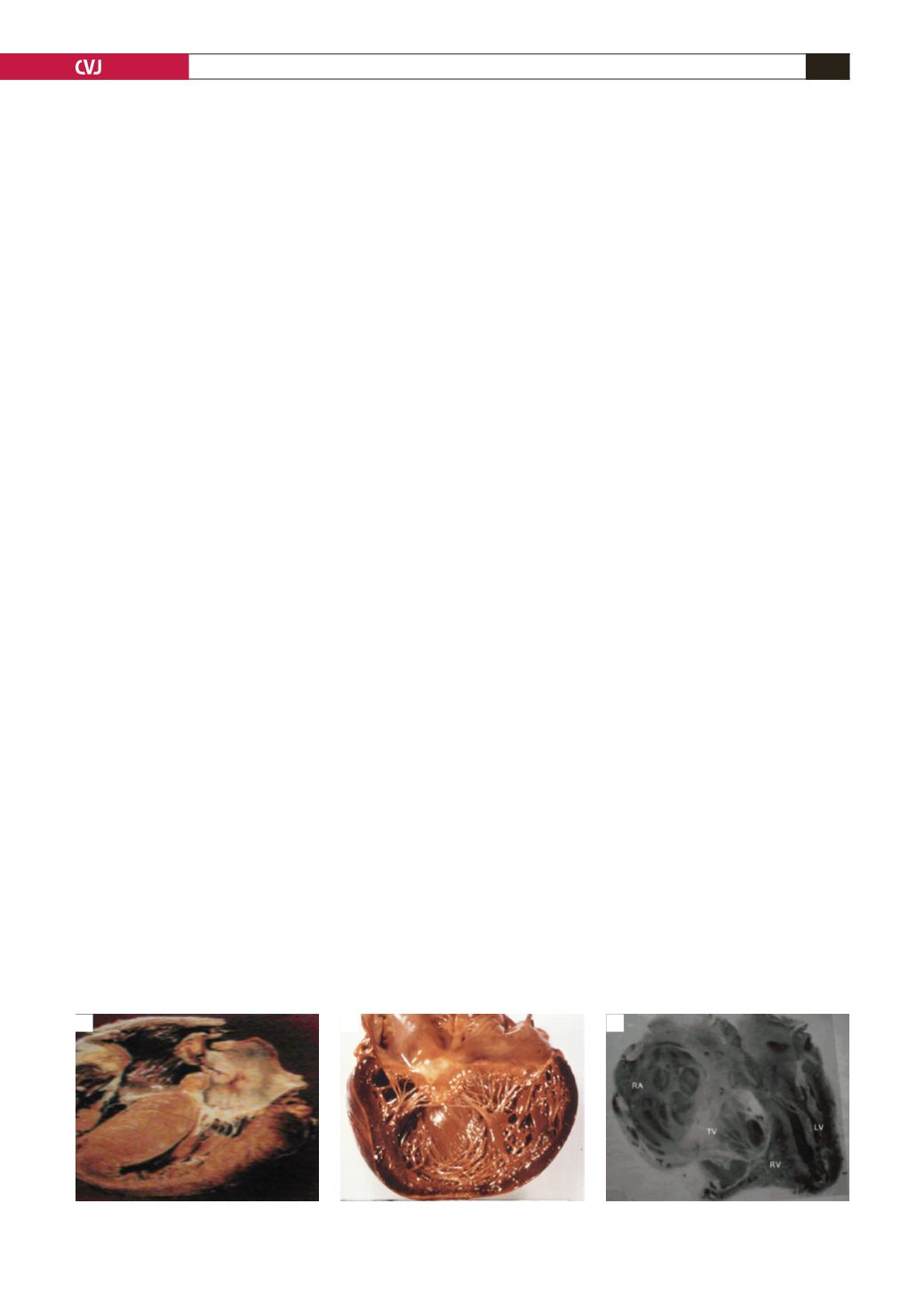
Fig 2.A. Hypertrophic cardiomyopathy; B. dilated cardiomyopathy; C. endomyocardial fibrosis.
A
B
C


