CARDIOVASCULAR JOURNAL OF AFRICA • Vol 23, No 10, November 2012
e10
AFRICA
Case Report
Single-stage repair of adult aortic coarctation and
concomitant coronary artery disease: an unusual
surgical approach through median sternotomy
MAHMUT MUSTAFA ULAS, KUMRAL ERGUN, GOKHAN LAFCI, NIHAT SEN, ADNAN YALCINKAYA,
AHMET IRDEM, KERIM CAGLI
Abstract
Surgical repair of postductal aortic coarctation associated
with severe coronary artery disease is in most cases a diffi-
cult decision to make. As staged procedures are associated
with a higher rate of morbidity and mortality, simultaneous
operative management of both pathologies is desirable. We
describe a case of a 51-year-old man who was referred to
our department for surgical treatment of postductal aortic
coarctation and concomitant coronary artery disease, which
we managed with single-stage surgery through median ster-
notomy.
Keywords:
single-stage surgical management, aortic coarcta-
tion, coronary bypass surgery
Submitted 28/12/10, accepted 3/9/12
Cardiovasc J Afr
2012;
23
:
e10–e12
DOI: 10.5830/CVJA-2012-061
Case report
A 51-year-old man was referred to our department with unstable
angina and uncontrolled hypertension. Echocardiography
demonstrated severe postductal aortic coarctation with 114
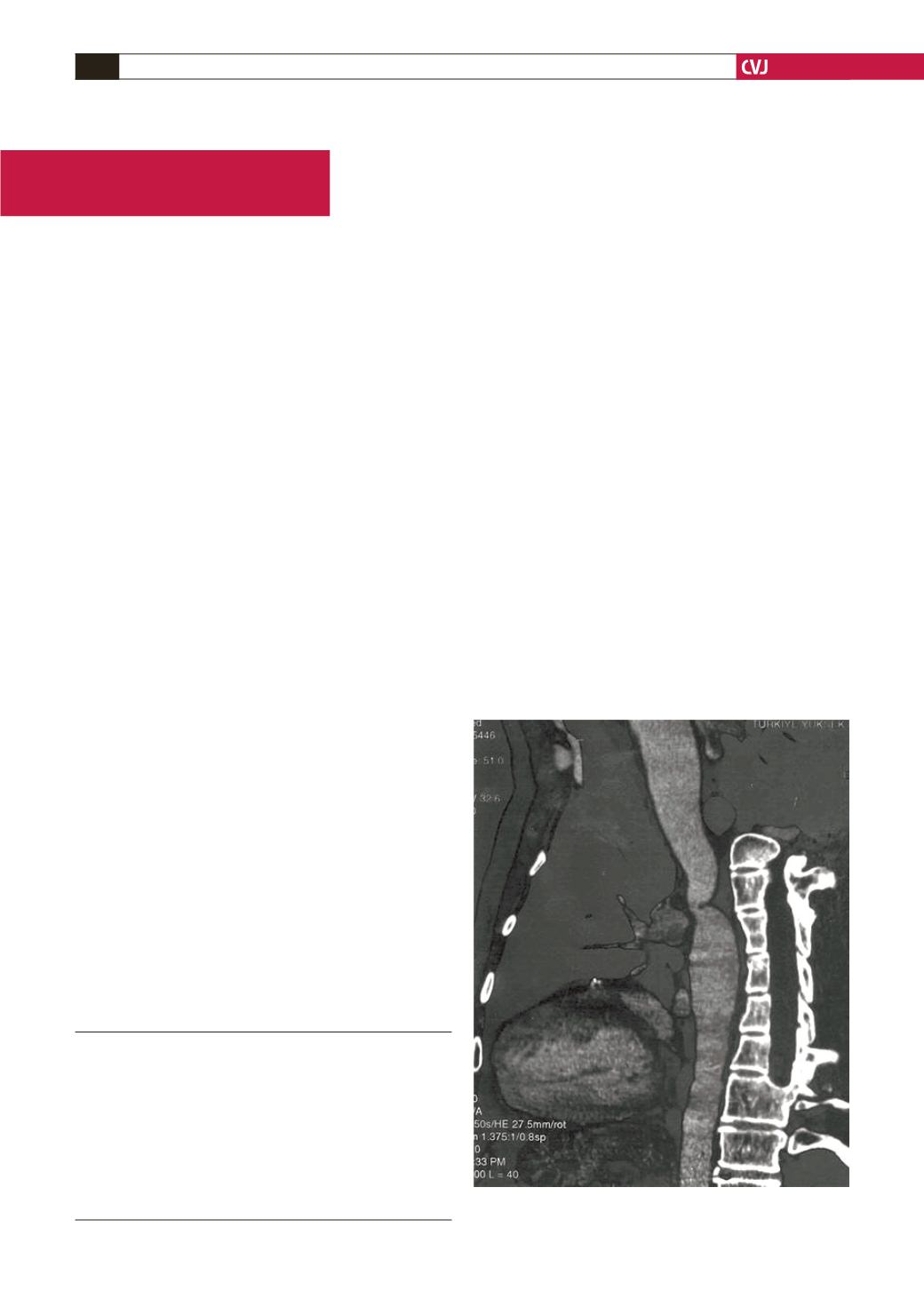
mmHg peak gradient at rest. CT angiography localised the aortic
coarctation (Fig. 1) and coronary angiography demonstrated
severe multi-vessel coronary artery disease.
We decided to perform coronary surgery first and then carry
out the coarctation repair. Surgery was performed via a standard
median sternotomy. The patient was anticoagulated with 1 mg/kg
of heparin. Cardiopulmonary bypass was instituted using right
atrial and ascending aortic cannulation.
Cold cardioplegic arrest of the myocardium was maintained
by infusion of cold cardioplegia into the aortic root and coronary
sinus. The patient was cooled down to 30°C rectal temperature.
After cross clamping, during the cooling period we performed
coronary surgery.
First, we carried out sequential graftings with the saphenous
vein. The distal anastomosis to the right posterior descending
artery was completed; then the proximal sequential anastomosis
to the right acute marginal artery, and finally the proximal
anastomosis to the ascending aorta was done.
Second, the distal anastomosis to the obtuse marginal branch
and the proximal sequential anastomosis to the diagonal artery
were carried out, and then the proximal anastomosis to the
ascending aorta. Finally, the (left internal thoracic artery)
LITA–LAD (left anterior descending artery) anastomosis was
Cardiovascular Clinic, Turkiye Yuksek Ihtisas Hospital,
Ankara, Turkey
MAHMUT MUSTAFA ULAS, MD
GOKHAN LAFCI, MD
ADNAN YALCINKAYA, MD
AHMET IRDEM, MD
KERIM CAGLI
Cardiology Clinic, Turkiye Yuksek Ihtisas Hospital, Ankara,
Turkey
KUMRAL ERGUN, MD
NIHAT SEN, MD
Fig. 1. CT angiography demonstrating localisation of the
aortic coarctation.


