CARDIOVASCULAR JOURNAL OF AFRICA • Vol 23, No 10, November 2012
AFRICA
e11
completed and a bulldog clamp was left on the LITA graft.
After all anastomoses were completed, the aorta was mobilised
extensively, the left pleura was opened, and a tape was passed
around the left pulmonary artery to retract it inferiorly. The
patient was turned to the right side and mini retractors were used
for maximum exposure. The arcus aorta was pulled up and to the
right, and the pulmonary artery was retracted inferiorly (Fig. 2).
After gentle retraction, the coarctation segment, left vagus
nerve, recurrent laryngeal nerve and ligamentum arteriosum
were seen. The ligamentum arteriosum was divided and over-
sewn. Large intercostal branches were identified and encircled in
preparation for snaring. The aorta was clamped just distal to the
left subclavian artery and distal to the coarctation. The aorta was
then incised longitudinally across the lesion and a wide Dacron
patch of appropriate size was sewn with fine, continuous prolene
sutures to the aortic edges (Fig. 3).
Cross-clamp time was 95 minutes. After declamping, cardio-
pulmonary bypass was discontinued uneventfully.
Two months later, the patient was asymptomatic and control
echocardiography revealed a mean 12 mmHg gradient (Fig. 4).
Discussion
Coarctation of the aorta generally presents in childhood.
However, a significiant number of patients will present with
primary coarctation later in life. A direct approach to repairing
coarctation may entail enormous difficulties in adults.
1
Severe
lung disease, large collateral formation, concomitant cardiac
pathologies, and lung dysfunction from a thoracotomy all present
technical challenges.
Surgery to repair only coarctation presenting in adulthood
is associated with significantly higher hospital and late
cardiovascular mortality.
2
The majority of these deaths are
caused by myocardial infarction, indicating the significant role
that myocardial disease plays in these patients.
The mortality and morbidity of a staged surgical approach is
significant. On the other hand, correction of the cardiac lesion
alone is associated with increased postoperative renal failure and
paraplegia as a result of inadequate perfusion of the distal organs.
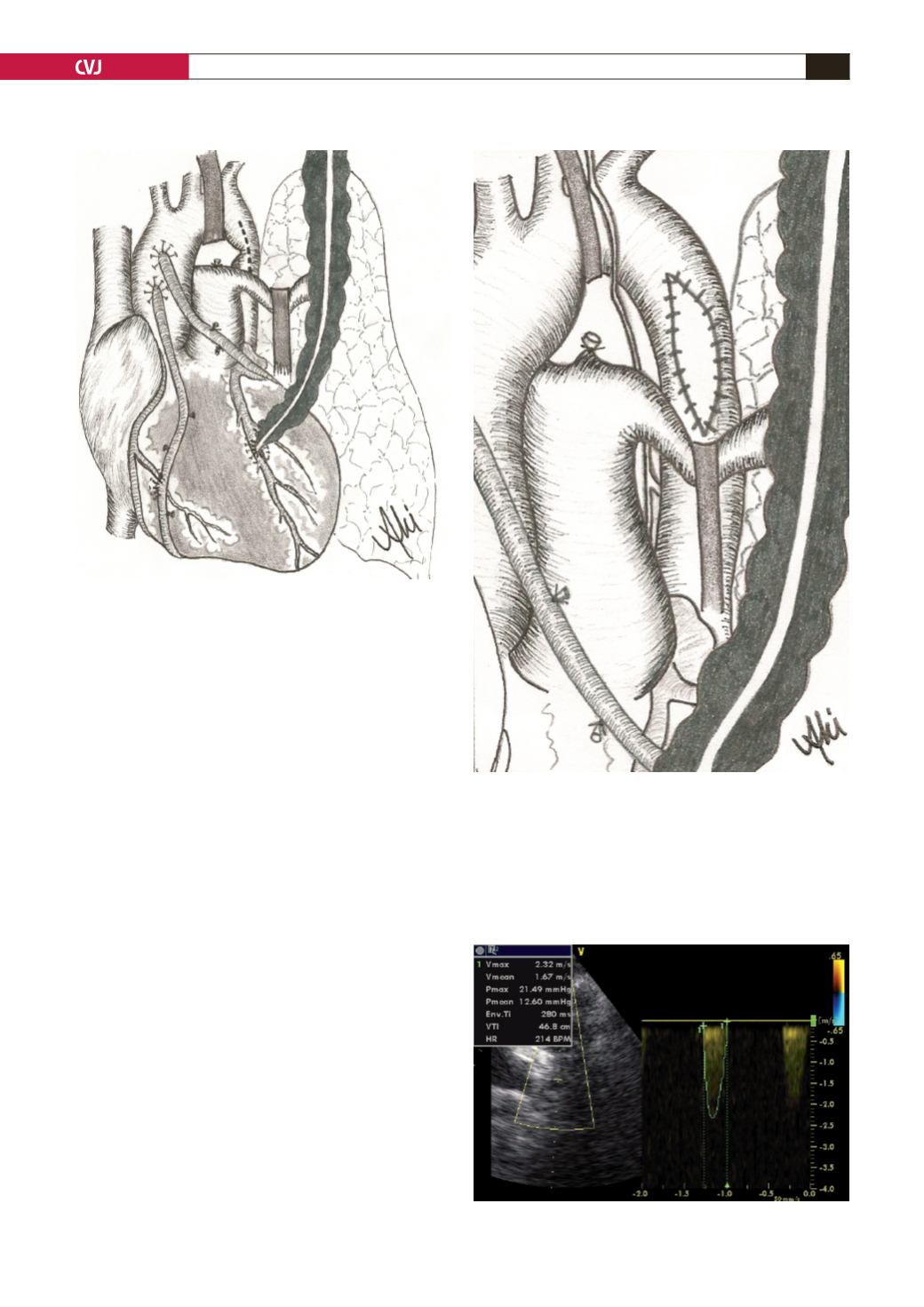
Fig. 2. A view of retraction of the arcus aorta and pulmo-
nary artery after coronary bypass.
Fig. 3. A view at the end of the operation.
Fig. 4. Postoperative echocardiographic findings.


