


















 26 / 66
26 / 66

CARDIOVASCULAR JOURNAL OF AFRICA • Volume 25, No 6, November/December 2014
276
AFRICA
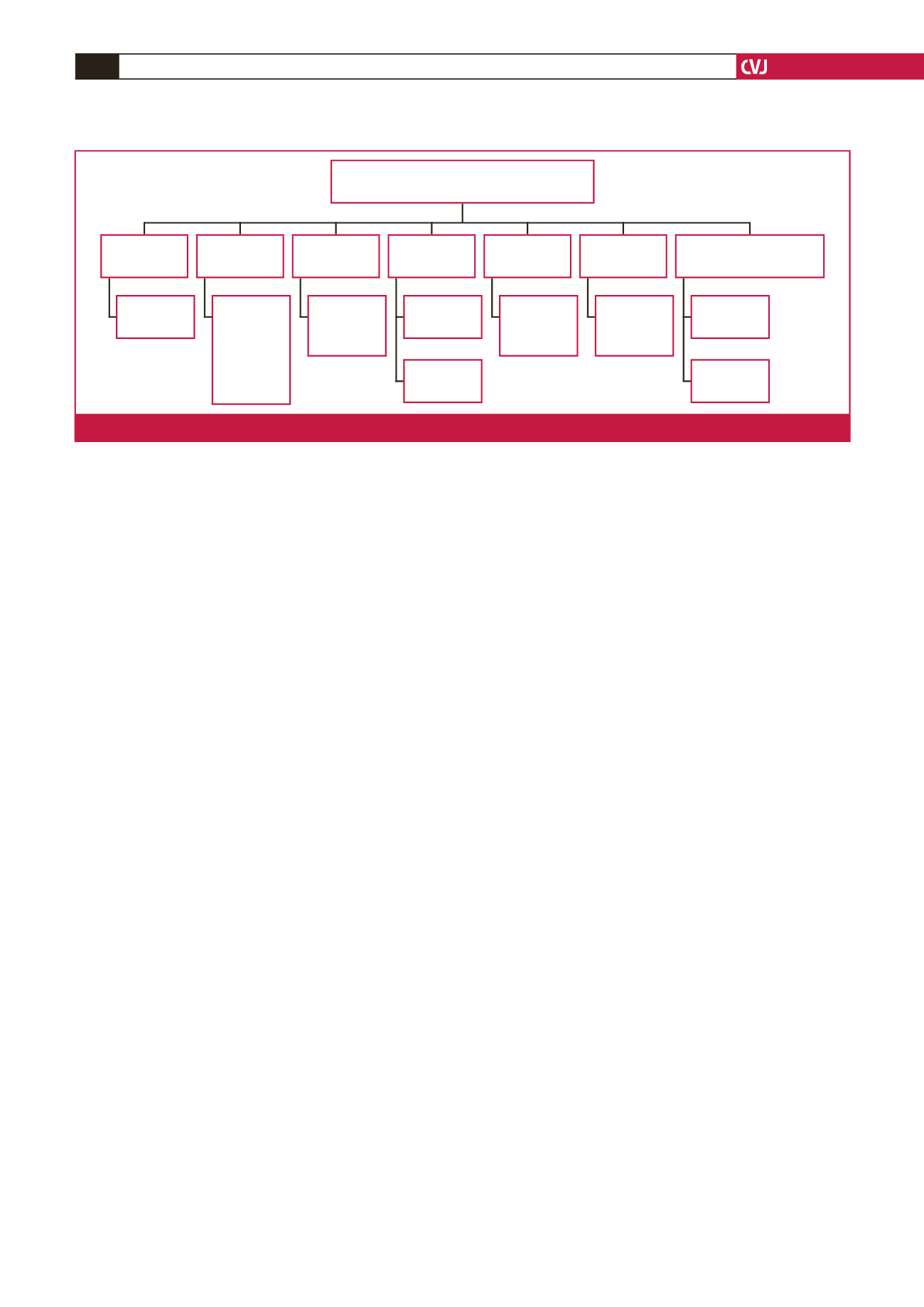
intake, sanitation, cleanwater supply, refrigeration, and electricity
access may influence HTN prevalence (Fig. 7). The ability to
make lifestyle changes may be related to SES, educational level
and economic development.
The economic development of both countries could raise both
countries’ SES, thus diminishing several factors contributing to
HTN prevalence. Sources of economic development in the
Gambia and Sierra Leone could include the many natural
resources present in these countries, which could be used for
economic self-sufficiency. With economic development, both
governments could offer funds for healthcare systems to lower
HTN prevalence.
Concerning HTN awareness, healthcare providers in
healthcare centres and religious leaders in religious institutions
could routinely make people aware of the disease, its progression
and burden, and its preventive means.
53
The government could
also establish national policies and programmes so that all
individuals, whether educated or not, would have an idea about
the existence of the disease HTN. In the Gambia, an improvement
in education and disease awareness is already underway.
42
Increased potassium (vegetable/fruit) intake and lowered
sodium intake are needed for protection against HTN.
18,20,46
The
high sodium (salt) intake is mainly due to the unavailability
of food preservation via refrigeration. Affordable electricity
systems could be established using the Berra Kunda waterfalls
in the Gambia on the border with Senegal, and the Bumbuna
waterfalls in Sierra Leone for hydroelectric power.
Chronic financial stress related to low SES and poor
economic conditions is potentially modifiable. A study in
Ghana and Cameroon suggested that religious institutions and
leaders should encourage the people to overcome their financial
problems and to start a recovery process from their stress.
53
Considering schistosomiasis, the Gambia and part of Sierra
Leone fall within the endemic region of the disease.
23,59
The main
prevention against such parasitic diseases is the improvement
of drinking water sources and sanitation facilities. Improper
sanitation and water supply are related to ascariasis, diarrhoea,
trachoma, schistosomiasis and other diseases.
60
An analysis
showed that cleaner water supplies led to a median reduction in
schistosomiasis morbidity rate of 69% for all studies and 77% for
four selected rigorous studies.
60
Study limitations
Study limitations include the gap in data collection in Sierra
Leone since the data were collected from 2001 to 2003 and in
2009. The data from the Gambia were only collected in 2000,
which may result in a smaller sample size from the Gambia
contributing to the findings of the study. In addition, combining
the data collected from both countries could potentially be a
weakness in the study, taking into account the fact that there
were some minor differences between the data collected from
the Gambia in 2000 and from Sierra Leone in 2001, as discussed
above. Finally, some ages were missing from the records,
resulting in the exclusion of these individuals from the statistical
analyses involving age.
Conclusion
HTN was highly prevalent in the Gambia and Sierra Leone. This
may have been due to low HTN treatment rates, low education
and awareness levels, low potassium and high sodium intakes,
and high stress levels, all of which are part of the persistently low
SES in both countries. Additional risk factors include smoking,
alcohol consumption, identified genetic loci and endemic
diseases. Lifestyle changes need to be instituted to lower this
high prevalence of HTN. Changes include raising the awareness
of the disease, initiating a stress-recovery process, finding
alternative ways to preserve foods and improving sanitation and
water supply sources.
References
1.
Mathenge W, Foster A, Kuper H. Urbanization, ethnicity and cardio-
vascular risk in a population in transition in Nakuru, Kenya: a popula-
tion-based survey.
BMC Public Health
2010;
10
: 569.
2.
Chobanian AV, Bakris GL, Black HR, Cushman WC, Green LA,
Izzo JL,
et al.
Seventh Report of the Joint National Committee on
Prevention, Detection, Evaluation, and Treatment of High Blood
Pressure.
Hypertension
2003;
42
(6): 1206–1252.
3.
Varon J. Treatment of acute severe hypertension: current and newer
agents.
Drugs
2008;
68
(3): 283–297.
4.
Kyrou I, Chrousos GP, Tsigos C. Stress, visceral obesity, and metabolic
complications.
Ann NY Acad Sci
2006;
1083
: 77–110.
Possible lifestyle changes to lower IITN
prevalence in the Gambia and Sierra Leone
HTN
treatment
Smoking
Psychosocial
status
Education
levels
Alcohol
consumption
Schistosomiasis & other
endemic diseases
Potassium/
sodium levels
Drug
expense
Smoking
cessation
therapies
Mental
recovery
process
Information
sessions
provided by
healthcare
providers
and relgious
leaders
Lower
alcohol
intake
Sanitation
Water
supply
Refrigeration
Electricity
access
Fig. 7.
Summary of possible lifestyle changes to lower HTN prevalence in the Gambia and Sierra Leone. HTN
=
hypertension.