


















 58 / 66
58 / 66

CARDIOVASCULAR JOURNAL OF AFRICA • Volume 25, No 6, November/December 2014
e4
AFRICA
supplementation with a daily dose of 100 mg for 11 days,
and continued administering multivitamins, including thiamine
hydrochloride 3.81 mg.
Follow-up echocardiography performed 15 days later revealed
normal LV systolic function with ejection fraction of 58%. The
patient’s condition was stabilised and he was transferred to the
general ward.
Discussion
Thiamine deficiency causes severe reduction in pyruvate
dehydrogenase activity, subsequently preventing conversion of
its substrate, pyruvate, into acetyl-CoA. This decrease in acetyl-
CoA produces deficiency in nicotinamide adenine dinucleotide,
resulting in a fall in cellular adenosine triphosphate (ATP).
3
The
accumulation of pyruvate and lactate thereby causes intense
vasodilatation due to peripheral arterio-venous shunts in the
skeletal musculature, with a resulting drop in systemic vascular
resistance and an increase in venous return.
4
Cardiac beriberi is a disorder of thiamine deficiency that
results in heart failure. Shoshin beriberi is a fulminant form
of this disease, designated as ‘a rapidly curable haemodynamic
disaster’,
5
and is characterised by hypotension, tachycardia and
lactic acidosis. The present case manifested classical signs of
shoshin beriberi.
Initially we suspected cardiogenic shock due to an acute
coronary event, supported by sudden hypotension, diffuse
ST-segment elevation on ECG and severe LV dysfunction on
portable echocardiography. However, CAG revealed no evidence
of acute myocardial infarction. At this point, a medical history
of long-standing TPN use, in conjunction with heart failure and
lactic acidosis was highly suggestive of a thiamine deficiency, or
shoshin beriberi.
In this case, we did not measure serum thiamine concentration
or red blood cell transketolase activity, the most commonly used
laboratory techniques for diagnosis of thiamine deficiency. These
tests are rarely performed in an emergency setting and the results
are often non-specific or inconclusive. Therefore, diagnosis of
shoshin beriberi is usually established by therapeutic response.
5-7
In the present case, a single dose of thiamine promptly
reversed both profound cardiovascular collapse and metabolic
acidosis, and this therapeutic response was diagnostic of shoshin
beriberi. According to previous reports, thiamine administration
improved the haemodynamics within hours and normalised
ECG changes within 24 hours in patients with shoshin beriberi.
6-8
In this case, ECG characteristically showed diffuse
ST-segment elevation in almost all the leads. There have been
two case reports showing ST-segment elevation mimicking acute
coronary syndrome in shoshin beriberi. One case showed a
focal ST-segment elevation, which can be also seen in Brugada
syndrome, suggesting autonomic nervous system abnormality
as a possible mechanism causing ST-segment elevation.
8
The
other case also revealed a focal ST-segment elevation and was
associated with electrolyte deficiency and metabolic alkalosis.
9
This is the first case report to demonstrate diffuse ST-segment
elevation in shoshin beriberi.
The exact mechanism leading to many different types of
ST-segment change and myocardial damage in shoshin beriberi
has not been revealed. Myocardial damage in the present case
was not likely, due to coronary artery disease. Hypotension
and secondary global coronary hypoperfusion may have played
a role in the subsequent cardiac dysfunction and myocardial
damage. Thiamine therapy may improve this and result in the
normalisation of ECG changes.
Myocardial energy depletion may induce myocardial damage
with ST-segment elevation because thiamine deficiency impairs
myocardial energy metabolism. Moreover, various studies
have suggested that activation of sarcolemmal ATP-sensitive
potassium channels by ischaemic ATP depletion may result in
ST-segment elevation.
10,11
Thiamine deficiency also induces ATP
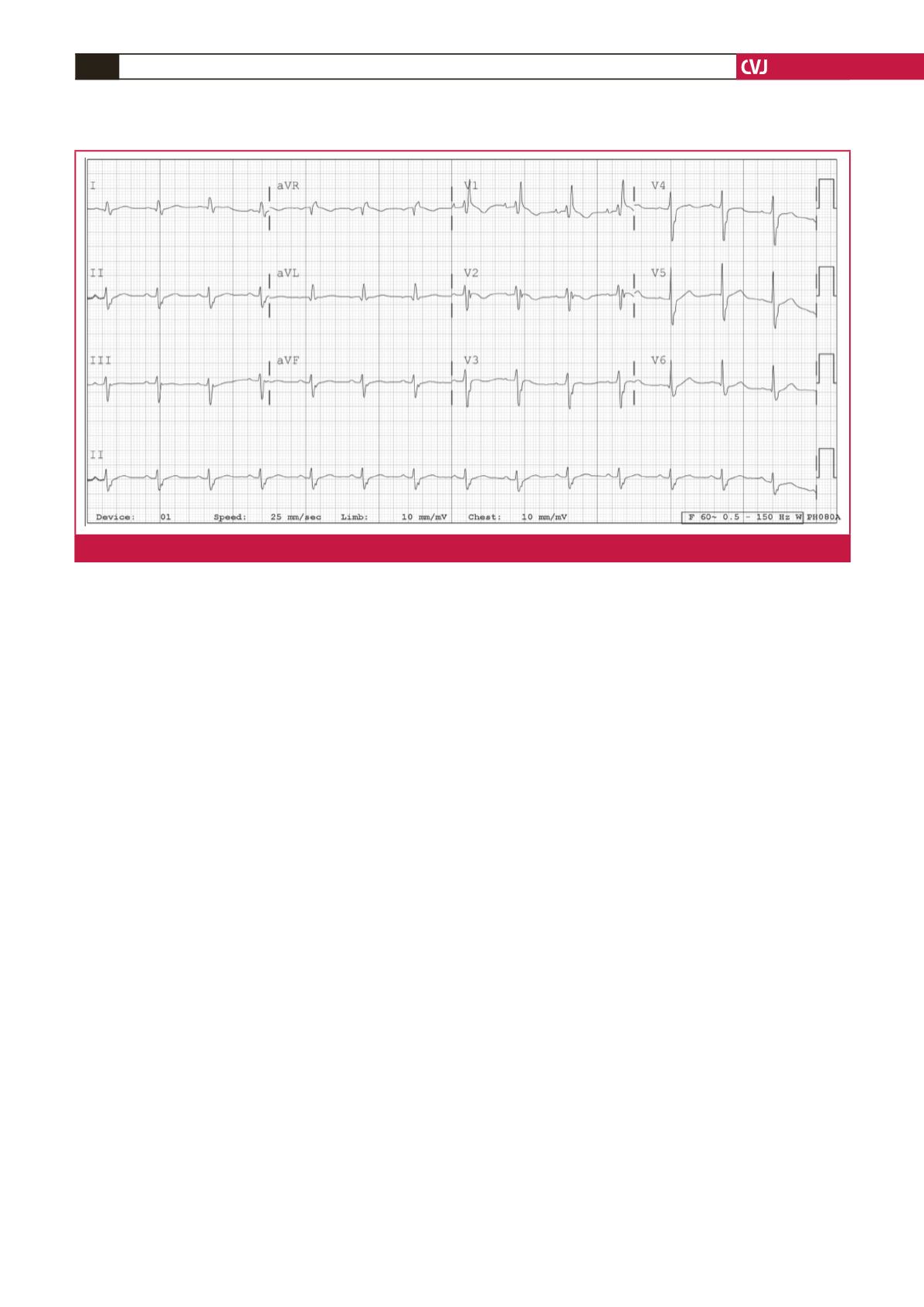
Fig. 5.
Five days after ICU admission, ST-segment elevation was normalised on ECG.