
















 20 / 67
20 / 67

CARDIOVASCULAR JOURNAL OF AFRICA • Volume 26, No 2, March/April 2015
66
AFRICA
femoral occlusion and died. Post-mortem examination showed
a large thrombus in the right atrium with evidence of multiple
pulmonary emboli.
Pedigree 1 clinical analysis
The younger brother of the proband, individual 1.III.2 (Fig.
1) had recurrent admissions over a seven-year period from the
age of 25 years, with recurrent isolated pleural effusions, both
right and left. Despite being transudates, the effusions were on
more than one occasion empirically treated as tuberculous. He
was also labelled ‘cor pulmonale’ but no lung disease that could
explain such a diagnosis was present. He has since died at the age
of 32 with severe right-sided congestion while being evaluated for
a heart transplant. The elder brother of the proband, individual
1.III.1 (Fig. 1), was asymptomatic at the time of most recent
contact, with an unremarkable clinical examination.
Their father, individual 1.II.2 (Fig. 1) presented at a similar
age as the proband, aged 25 years (in 1978). With the clinical
emphasis on right-sided heart failure, he had a sequential series
of diagnoses, namely pulmonary hypertension with cardiac
failure, CP due to TB, since TB and its various manifestations
are extremely common in South Africa,
8
and finally RCM
(sarcoidosis/amyloidosis). A first cardiac catheterisation was
believed to be compatible with CP, but a note drew attention to
the absence of an apparent thickened pericardium.
His course was complicated by the onset of atrial fibrillation
and he died, aged 28 years, as a consequence of recurrent
embolic phenomena with cerebrovascular accidents on more
than one occasion, despite anticoagulation. Material from a
pericardial, endocardial or tongue biopsy as a possible source of
DNA for a molecular diagnosis could not be traced.
Clinical features of the proband in pedigree 2
(Individual 2.II.3)
Individual 2.II.3 (Fig. 3) presented with signs and symptoms of
biventricular cardiac failure at age 15 years. Although clubbed
feet were surgically corrected soon after birth, no cardiac
anomalies were documented at that time. An electrocardiogram
showed sinus rhythm with peaked P waves and a chest X-ray
demonstrated a widened cardiothoracic ratio with evidence of
pulmonary vascular congestion. His echocardiogram showed
markedly dilated atria and non-dilated, small ventricles (Table 2).
He was treated for heart failure on admission and was discharged
on anti-failure and anti-coagulation medication.
Pedigree 2 clinical analysis
The nuclear family, comprising the parents, an older sister and
older brother (Fig. 3), were normal on physical examination,
electrocardiography and echocardiography (Table 2).
In-depth echocardiographic analysis
Echocardiographic findings are summarised in Table 2. In
pedigree 1, all the siblings had extremely enlarged atriae with
relatively small end-diastolic left ventricles with good ejection
fractions (Fig. 2). However, in the proband (1.III.3, Fig. 1),
long-axis systolic function was compromised, as exemplified
by the averaged septal and lateral systolic annular velocities
measured with pulse-wave tissue Doppler (s
′
septal and s
′
lateral, respectively), while in the younger (1.III.2, Fig. 1)
and older brother (1.III.1, Fig. 1) it was preserved. In the
case of right ventricular systolic function, the longitudinal
tricuspid annular-plane systolic excursion (TAPSE) was only
7 mm, suggesting significant impairment of longitudinal right
ventricular shortening. However, this was slightly better in
the symptomatic brother (10 mm) and relatively good in the
asymptomatic brother (17 mm).
Severe diastolic dysfunction with raised filling pressures was
present in the proband, as shown by the restrictive transmitral
filling pattern (transmitral E-wave deceleration time 96 ms) and
E/e
′
lateral
>
10, in addition to the atrial dilatation. In individual
1.III.2, the left ventricular diastolic parameters were measured
with the patient in atrial fibrillation and were impaired. In the
older, asymptomatic brother (1.III.1, Fig. 1), the left ventricular
diastolic function was significantly impaired with early diastolic
lateral annular long-axis velocities of 7 cm/s. Filling pressures
were elevated as evidenced by a restrictive transmitral filling
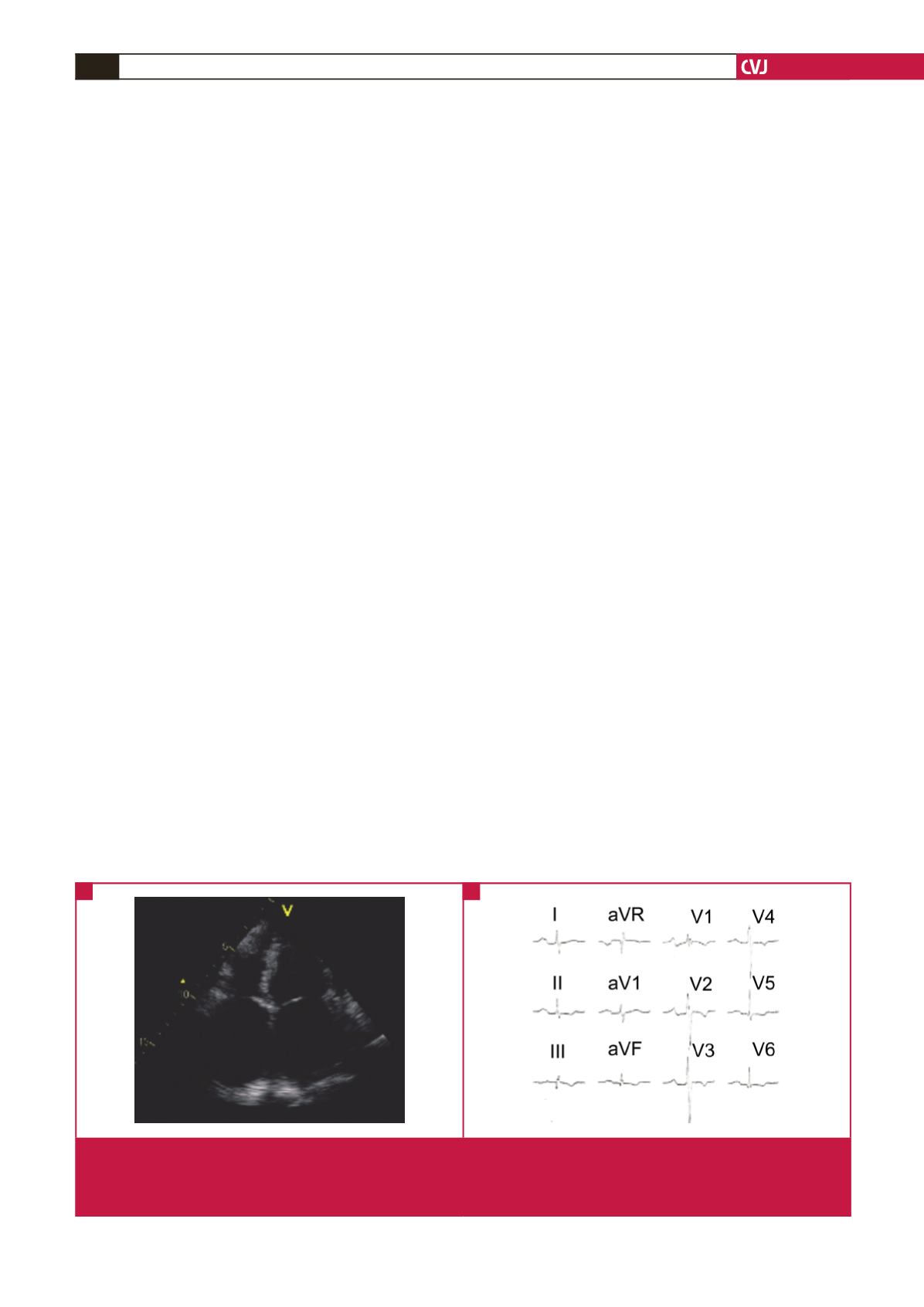
Fig. 2.
Clinical features of RCM in individual 1.III.3 affected by the p.Leu144His mutation in
TNNI3
. (A) Apical four-chamber echocar-
diogram in diastole with marked bi-atrial dilatation, which was captured using a GE Vivid 7 ultrasound machine. (LA, left
atrium; LV, left ventricle; RA, right atrium; RV, right ventricle). (B) 12-lead electrocardiogram in sinus rhythm with P-mitrale
and partial right bundle branch block, which was captured using a GE Mac 1200: ECG/EKG system.
A
B