
















 48 / 67
48 / 67

CARDIOVASCULAR JOURNAL OF AFRICA • Volume 26, No 2, March/April 2015
94
AFRICA
counselling, as this case report has shown. An experienced
physician would have avoided the long in-hospital stay that this
patient had without any specific management. Refusing to be
discharged without medical indications is a manifestation of the
patient’s altered cognitive function, which had significant cost
implications. Indeed, ‘paying for care’ in low-resource settings
has great financial implications.
The life-threatening conditions of the patients in three reported
cases would have impacted negatively on their QoL. This would
have been a source of significant stress to the family.
9,10
Lessons from the guidelines
The most common electrical mechanism of cardiac arrest
is ventricular fibrillation or pulseless ventricular tachycardia,
but substantial numbers of cases of cardiac arrest begin as
severe bradyarrhythmias, asystole or ventricular tachycardia.
The guidelines
6,11
state the following:
•
Cardiopulmonary resuscitation should be implemented after
contacting a response team (class I, level of evidence A).
•
For victims of ventricular tachyarrhythmic mechanisms of
cardiac arrest who have recurrences after maximal defibril-
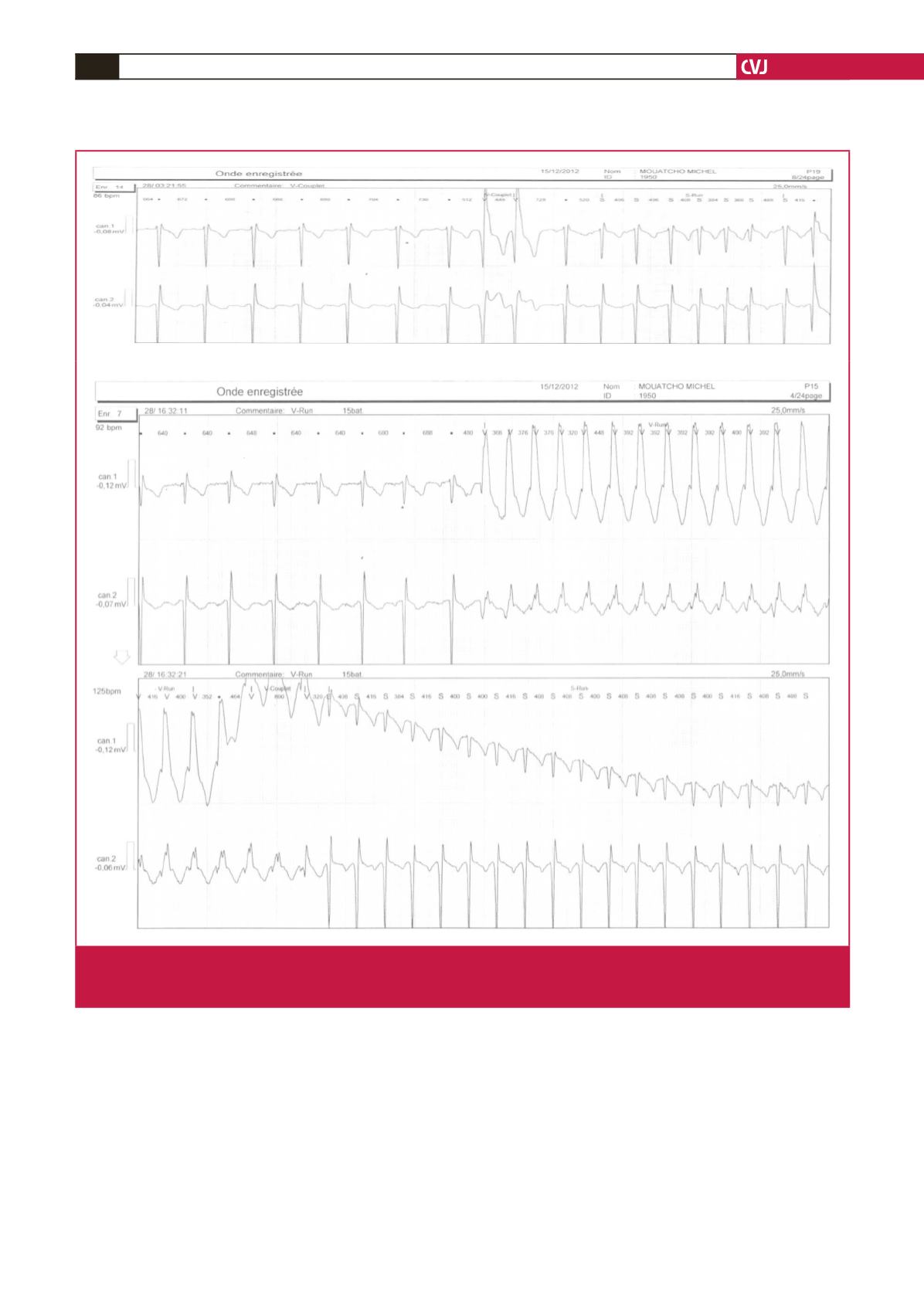
Fig. 3.
ECG recordings showing premature ventricular contractions a few days after the patient had experienced SCA. Top: two-lead
recording showing paired premature ventricular contractions. Bottom: one-lead recording registered sustained ventricular
tachycardia, which was amended by external electrical cardioversion.