
















 47 / 67
47 / 67

CARDIOVASCULAR JOURNAL OF AFRICA • Volume 26, No 2, March/April 2015
AFRICA
93
of interest regarding the epidemiology and management of SCA
in SSA: aetiology, ability to perform CPR, healthcare facilities,
physician’s awareness to manage such patients and QoL of
resuscitated victims living without complete diagnostic work-up.
Coronary artery disease (CAD) is the most common cause
of SCA in western countries.
7
The pathogenesis of acute
coronary syndrome (ACS) has changed and more cases of MI
with ‘normal’ coronaries, such as in this case report, are seen
with angiography.
8
Almost all leading causes of SCA have been
described in sub-Saharan Africa (Table 1). However, many
patients who have died suddenly and in whom the diagnosis of
MI was suspected, were not fully investigated.
This case report is a typical scenario of incomplete work-up in
a remote African setting. Detailed cardiac work-up including 2D
echo, CT angiography, coronary angiography and cardiacMRI was
possible abroad. In this framework, the diagnosis of MI-related
ventricular tachycardia was confirmed. Furthermore, it is worth
noting that this case of SCA due to ischaemic cardiomyopathy
without coronary atherosclerosis has not been reported in SSA.
As data of SCA are limited in Africa, secondary prevention
through the introduction of widespread CPR is not frequently
done. Therefore resuscitated victims of cardiac arrest are rare,
their long-term outcome remains unknown, and the aetiology
needs to be established.
The patient in this case is still alive, courtesy of BLS
manoeuvres provided by bystanders. This demonstrates that
even in remote, low-resource settings, SCA can be aborted
through CPR attempts.
Given the cost of diagnostic and therapeutic tools used for
patients experiencing arrhythmic disorders, the management
of patients is in its early stages in SSA. Although a few
SSA countries now have the availability of echocardiography,
stress ECG, Holter monitoring, coronary angiography, CT
angiography and MRI, the majority in this part of the world
cannot provide their population with such advanced healthcare
facilities.
Therefore, physicians who seldom treat SCA patients
are not fully competent to provide adequate treatment and
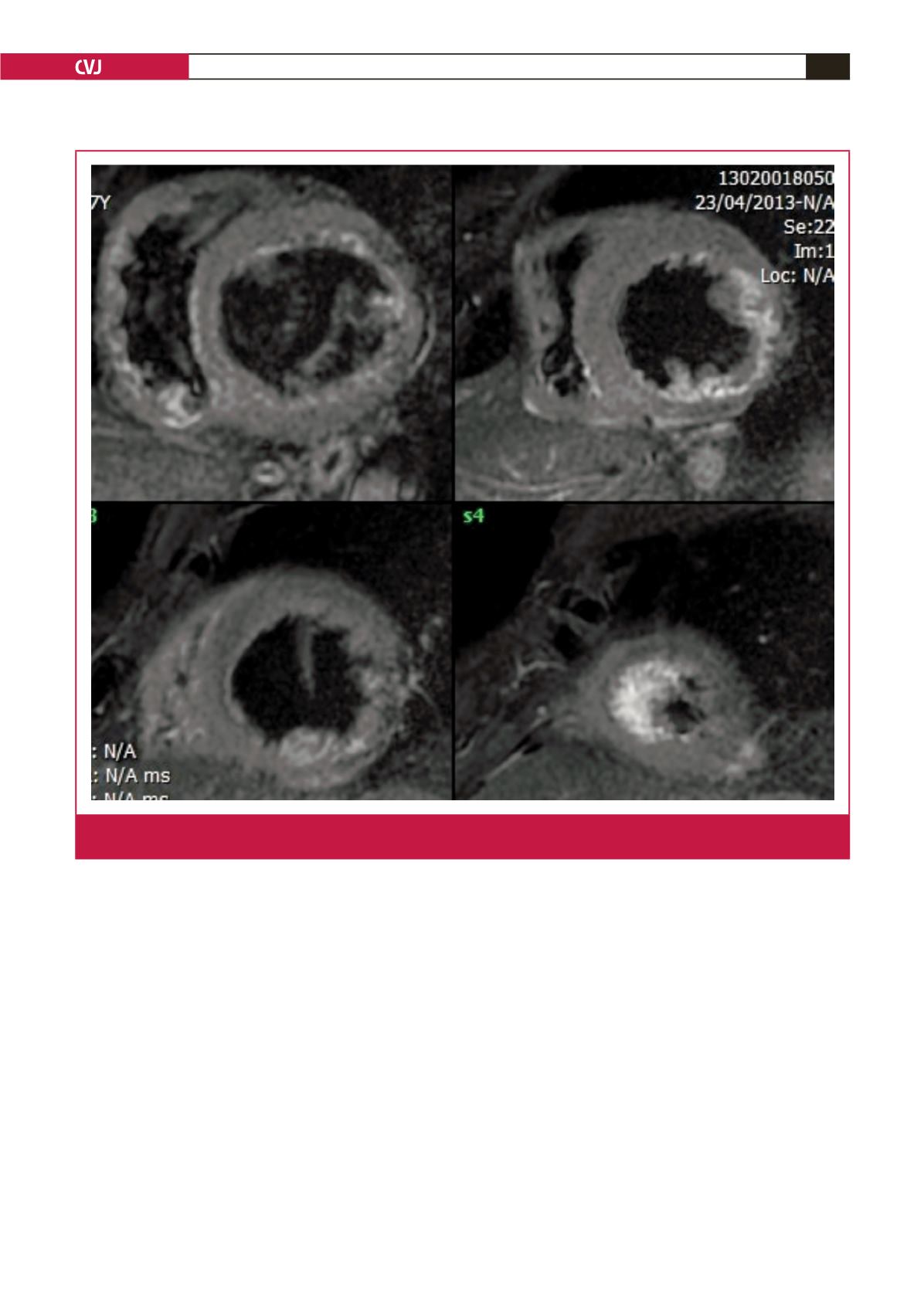
Fig. 2.
Apical view of cardiac magnetic resonance imaging showed antero-lateral and infero-latero-basal and mild left ventricular
akinesia, in conjunction with transmural late enhancement in the akinetic segments with a thickness of
<
5 mm.