
















 91 / 102
91 / 102

CARDIOVASCULAR JOURNAL OF AFRICA • Volume 27, No 3, May/June 2016
AFRICA
e9
Transcatheter intervention in a child with scimitar
syndrome
Zhouping Wang, Xiaoyi Cai
Abstract
Scimitar syndrome is a rare congenital heart disease char-
acterised by anomalous pulmonary venous drainage to the
inferior vena cava, aortopulmonary collaterals, hypoplasia
of the right lung and intracardiac defects. Surgical correction
remains the gold-standard therapy. However, non-surgical
intervention has been reported effective in selected cases with
scimitar syndrome. We report on a one-year-old boy with
scimitar syndrome who underwent stepwise transcatheter
intervention as an alternative treatment. Embolisation of
the aortopulmonary collaterals and occlusion of the atrial
septal defect were performed using detachable coils and an
Amplatzer septal occluder, respectively. The patient’s post-
cathetherisation course was uneventful. The right cardiac
chamber and pulmonary arterial pressure returned to normal
during follow up.
Keywords:
scimitar syndrome, congenital heart disease, tran-
scatheter intervention
Submitted 1/7/15, accepted 17/1/16
Published online 8/6/16
Cardiovasc J Afr
2016;
27
: e9–e11
www.cvja.co.zaDOI: 10.5830/CVJA-2016-004
Scimitar syndrome is a rare congenital anomaly consisting of
anomalous pulmonary venous drainage from the right lung to
the inferior vena cava (IVC), hypoplasia of the right lung, cardiac
dextroposition, and malformation of the right pulmonary artery
and aortopulmonary collaterals (APC) supplying the lower lobe
of the right lung.
1-3
Its prevalence is low and is estimated at two
out of every 100 000 live births.
4
The clinical presentations are quite diverse, ranging from
severe congestive heart failure in infancy to mild symptoms in
childhood, and depend greatly on the extent of left-to-right
shunting from partially anomalous pulmonary venous drainage
and aortopulmonary collateral flow.
5,6
Scimitar syndrome has
two types. One is the adult form, which is usually asymptomatic
and not associated with other cardiac disorders. The other type is
the infantile form, presenting with signs and symptoms of severe
pulmonary hypertension, associated cardiac malformations, and
large systemic collateral arteries feeding the right lung in the
first weeks of life. Transcatheter embolisation of the APC and
repair of co-existing cardiac defects may improve symptoms and
decrease pulmonary arterial pressure in symptomatic patients.
7-8
Herein we describe a boy with scimitar syndrome who had
obvious clinical improvement and pulmonary arterial pressure
drop after transcatheter embolisation of the APC and atrial
septal defect closure.
Case report
A one-year-old, 9.5-kg male was admitted to our hospital
(Guangzhou Women and Children Medical Centre, China) with
tachypnoea. He had a history of recurrent pneumonia, sweating
and growth retardation.
On admission, a physical examination revealed grade II/VI
systolic murmur at the left sternal border. Moreover, cardiac
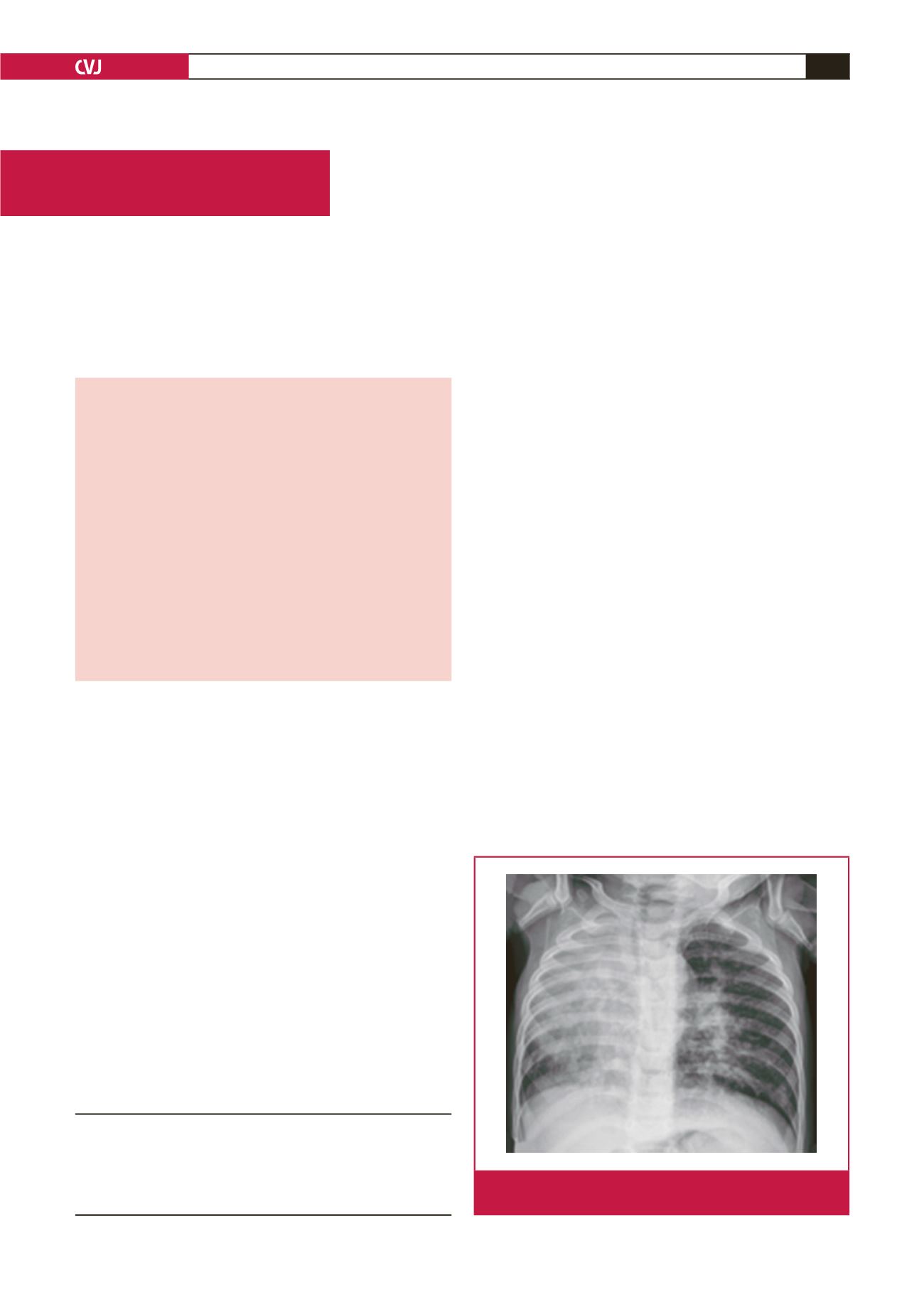
dextropositionanda radiopaque right hemithoraxwere confirmed
on a chest X-ray examination (Fig. 1). Echocardiography
showed an enlarged right cardiac chamber, partially anomalous
pulmonary venous drainage, an 8-mm secundum atrial septal
Department of Cardiology, Guangzhou Women and
Children’s Medical Centre, Guangzhou, Guangdong
Province, China
Zhouping Wang, MD,
freebirdwzp@sohu.comXiaoyi Cai, MSc
Case Report
Fig. 1.
Chest X-ray showing cardiac dextroposition and radio-
paque right hemithorax.