
















 95 / 102
95 / 102

CARDIOVASCULAR JOURNAL OF AFRICA • Volume 27, No 3, May/June 2016
AFRICA
e13
the myocardium.
6
The mortality rate from TCMP is lower than
that of acute myocardial infarction. In-hospital mortality is
quite low, at 1–2%.
1,4
The complications include apical thrombus
formation, cardiac rupture, embolism and conduction defects.
7
De Gregorio
et al
. (2008) reported intracavitary thrombus
in 2.5% of the patients with TCMP, and stated that 33%
of these patients may have thromboembolic complications.
8
However, thromboembolic events may occur even in patients
receiving anticoagulant treatment.
7
Myocardial necrosis and
haemorrhage are feared limitations in treatment decisions.
9
Surgical thrombectomy has drawbacks, such as decreasing
the ejection fraction in the early post-surgical period, and the
increased risks of anaesthesia and operational stress for patients
with TCMP.
10,11
Conclusion
This patient’s outcome shows that anticoagulant treatment with
warfarin is an effective, conservative treatment option. Despite
ongoing debate, it would be beneficial to consider warfarin in
individualised treatment, and the decision should be made with
consideration of the features of intracavitary thrombus.
Fig. 2.
Coronary angiography with normal coronary angio-
graphic findings.
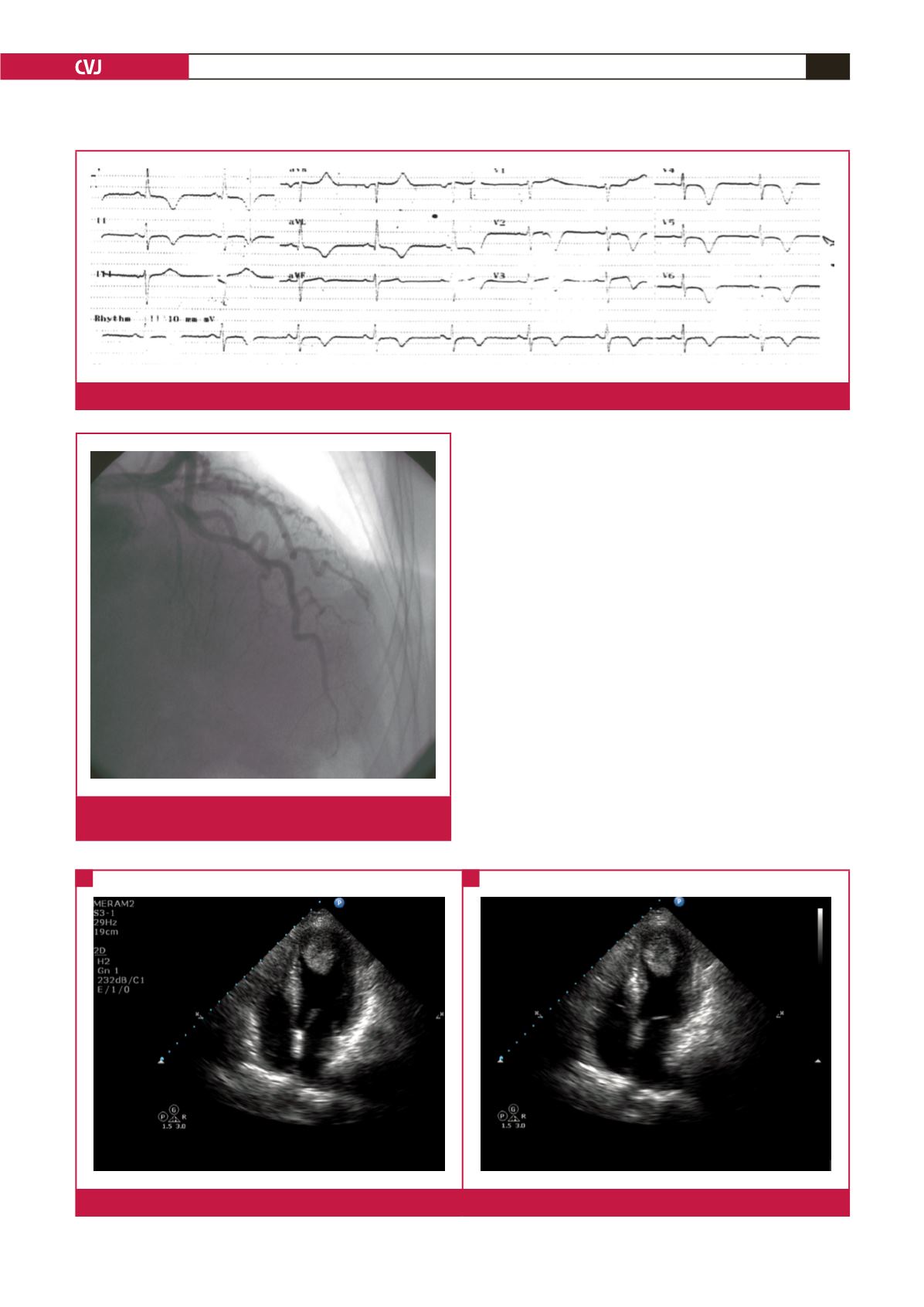
Fig. 3.
Initial echocardiography showing apical ballooning and apical thrombus in the diastolic and systolic phase.
A
B
Fig. 1.
Admission ECG showing ST–T changes.
Diastole
Systole