
















 88 / 102
88 / 102

CARDIOVASCULAR JOURNAL OF AFRICA • Volume 27, No 3, May/June 2016
e6
AFRICA
therapy. The reference diameter of the RCA was 6.2 mm (Fig.
3). The patient received repeated thrombus aspiration, but large
thrombi still remained in the RCA. We decided to continue the
enoxaparin therapy for several days instead of stenting, due to
the large diameter of the RCA.
After 10 days of enoxaparin therapy, the patient complained
of epistaxis and her platelet count was 11 000 cells/
μ
l. We stopped
the enoxaparin injection and checked the coagulation profile and
heparin–platelet factor 4 antibody. The anti-factor Xa activity
was not measured. The coagulation profiles were normal, but
the heparin–platelet factor 4 antibody was strongly positive
and she was a heparin-naïve patient. After discontinuation of
enoxaparin, the platelet count recovered to 49 000 cells/
μ
l on the
first day and 117
×
10
3
cells/
μ
l on the second day. Fortunately,
there were no adverse cardiac events.
The second follow-up CAG and IVUS were performed on the
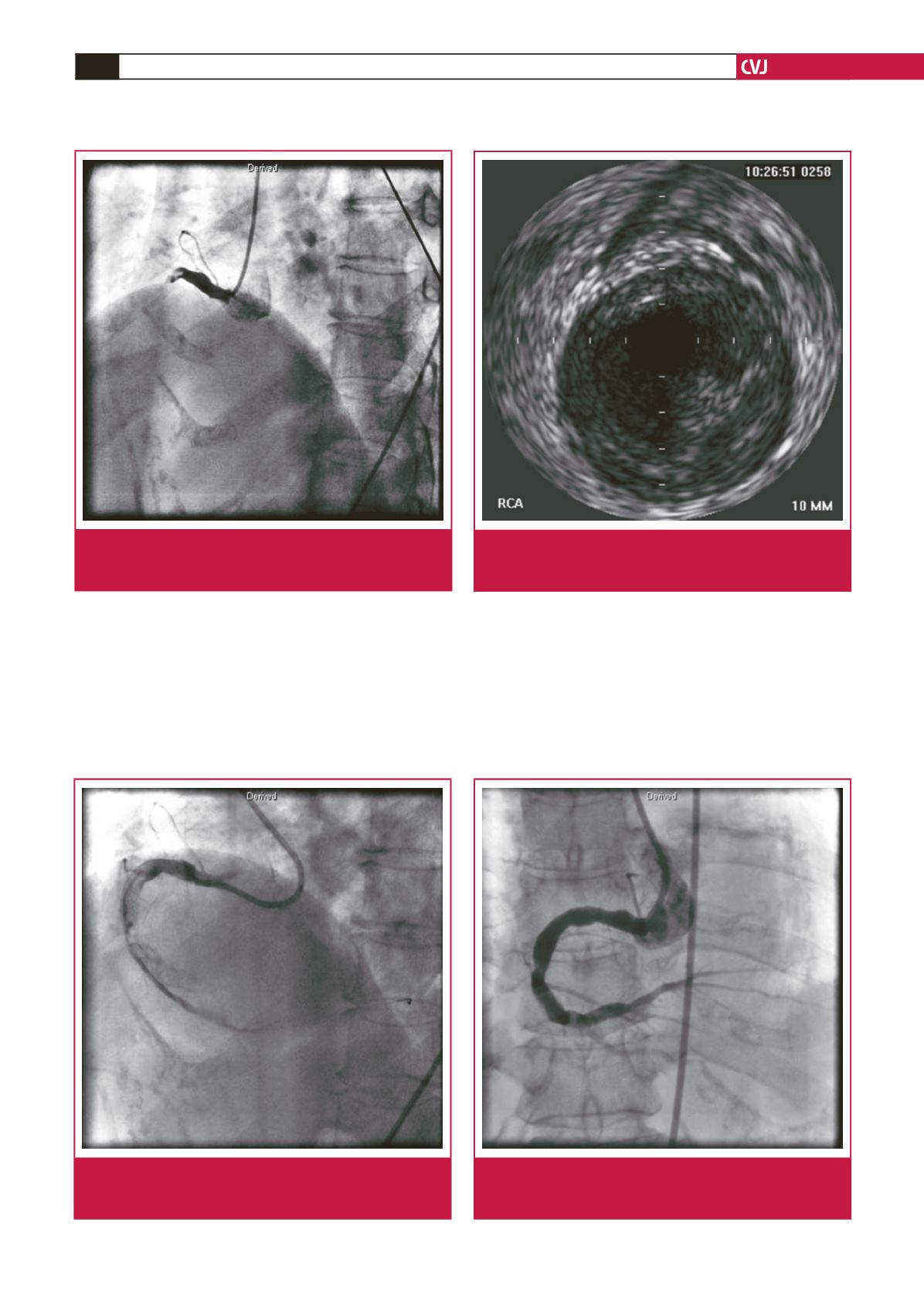
Fig. 3.
Intravascular ultrasound (IVUS) revealed thrombi still
present in the large RCA. The reference diameter of
the RCA was 6.2 mm.
Fig. 4.
The follow-up CAG was performed on the 15th day
after admission and revealed resolution of the thrombi
in the RCA, with improved distal flow.
Fig. 1.
Emergent coronary angiogram (CAG) revealed total
thrombotic occlusion of the proximal right coronary
artery (RCA).
Fig. 2.
The follow-up CAG revealed thrombi still present in
the large RCA, even after seven days of enoxaparin
therapy.