
















 98 / 102
98 / 102

CARDIOVASCULAR JOURNAL OF AFRICA • Volume 27, No 3, May/June 2016
e16
AFRICA
A graph of oesophageal passage was done on postoperative
day 12 with iohexol (Omnipaque
®
, Nycomed, Oslo, Norway)
contrast agent and no leakage was observed (Fig. 1C, D). The
patient was discharged uneventfully on the 15th day after the
operation.
Discussion
We could not find any cases in the literature reporting aortic
rupture during rigid oesophagoscopy. Therefore we report on
this case with a view to preventing such complications in other
patients.
Foreign body ingestion is frequently seen in early childhood.
Peristaltic transmission of these foreign bodies to the stomach
may be challenging due to anatomical constriction of the
oesophagus.
4,5
In these cases, endoscopic (10–20%) or surgical
(1%) removal may be required.
4,5
However, both the foreign body
and the endoscope used for removal of the object could lead to
aortic wall injury.
3,5
Incidence of oesophageal rupture is reported at 0.1 to 1.9%
during rigid oesophagoscopy.
6
Aorto-oesophageal fistula is a
rare but fatal (40–60%) complication of foreign body ingestion.
The common site of aortic injury is at the second constriction of
the oesophagus, which has a relatively narrow lumen due to the
cross-over of the left primary bronchus and aortic arch.
3
Aortic rupture of the oesophagus usually has a fatal course,
particularly with spontaneous rupture of the aorta. He
et al
.
reported sudden death due to ruptured pseudo-aneurysms into
the oesophagus.
7
However, iatrogenic injuries of the aorta can
be more easily controlled than unforeseen events. Therefore,
pre-operative staging of the condition and planning of the
procedure is important to avoid fatal outcomes.
Similar injuries have been reported with other thoracic
interventions, such as spinal instrumentation and surgical
and endovascular aortic repair techniques described for
treatment of complications.
8
However, direct aortic injury
during oesophagoscopy is not reported as frequently as other
complications. The majority of reports mention oesophageal
rupture due to foreign body removal with oesophagoscopy.
1,2
Oesophageal perforations may cause fatal outcomes due
to mediastinitis and fulminant sepsis, which could prevent
oesophageal repair.
1,2
However, in combination with aortic
rupture, this may become an emergency situation. An aorto-
oesophageal fistula will usually occur after neglect of an ingested
foreign body, as the oesophagus compresses the object, which
irritates the oesophageal wall. This condition may develop over
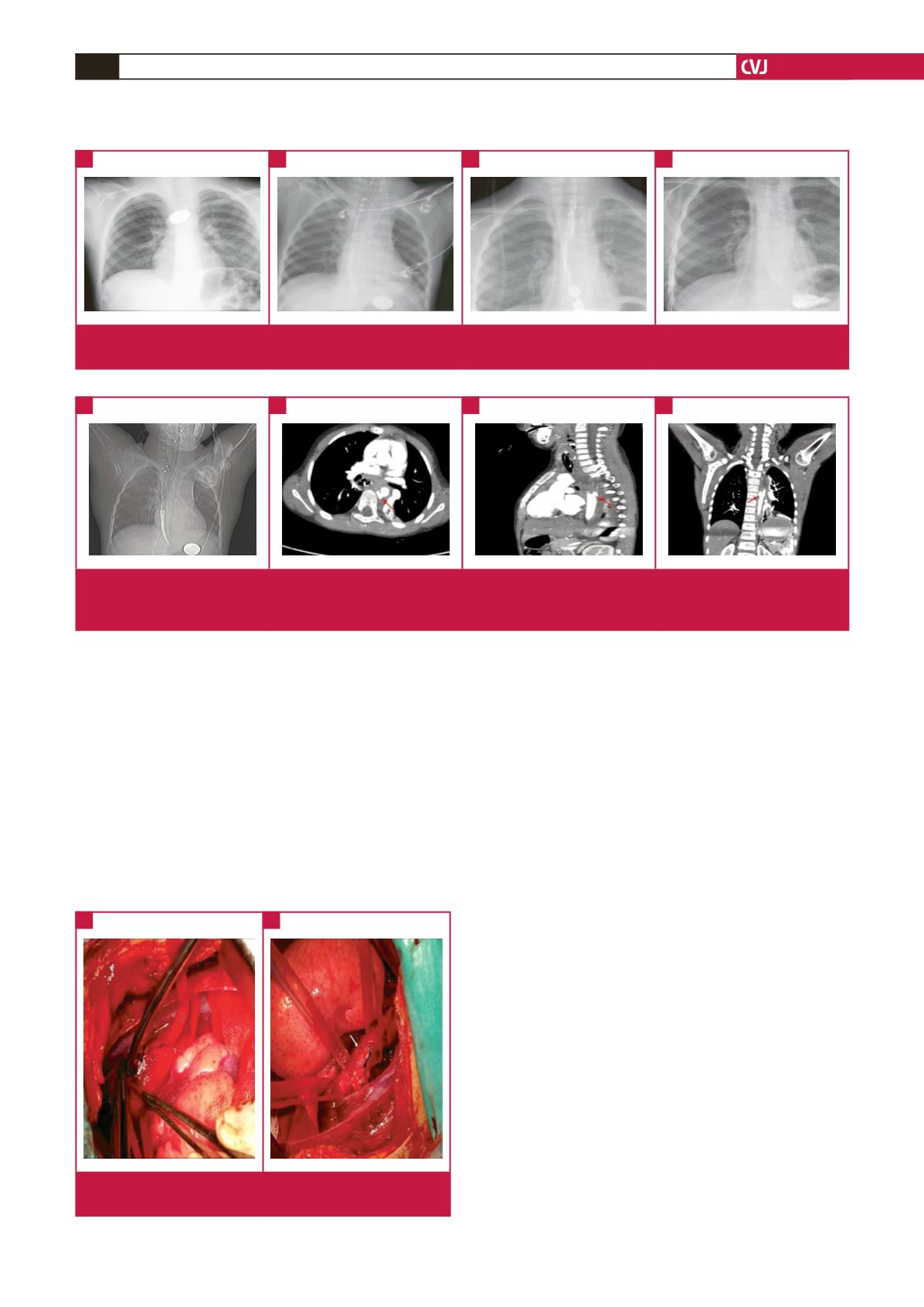
Fig. 1.
A. Chest radiography showing the first position of the ingested coin. B. Reposition of the coin in the stomach and visualisation
of the achalasia balloon. C, D. Oesophageal radiographs on postoperative day 12.
A
B
D
C
Fig. 2.
A. Achalasia balloon placed in the oesophagus. B. Contrast extravasation (red arrow) from aortic rupture (axial view). C.
Contrast extravasation (red arrow) from aortic rupture (sagittal view). D. Contrast extravasation (red arrow) from aortic
rupture (coronal view).
A
B
D
C
Fig. 3.
A. Adventitial haematoma from the aortic injury. B.
Aortic injury repaired with pledgeted suture.
A
B