
















 72 / 76
72 / 76

CARDIOVASCULAR JOURNAL OF AFRICA • Volume 28, No 1, January/February 2017
e2
AFRICA
Discussion
The cardiac phenotype of HCM shows great diversity in the
degree and pattern of hypertrophy, such as asymmetric, concentric
or apical.
1
Asymmetric hypertrophy is often located in the whole
IVS, not in a focal site. To the best of our knowledge, there has
been only one case reported that revealed isolated posterobasal
left ventricular free wall hypertrophy, which has extended the
morphological diversity of HCM.
2
In our case, the basal IVS not only showed hypertrophy,
but also exhibited an angulation deformity, which has never
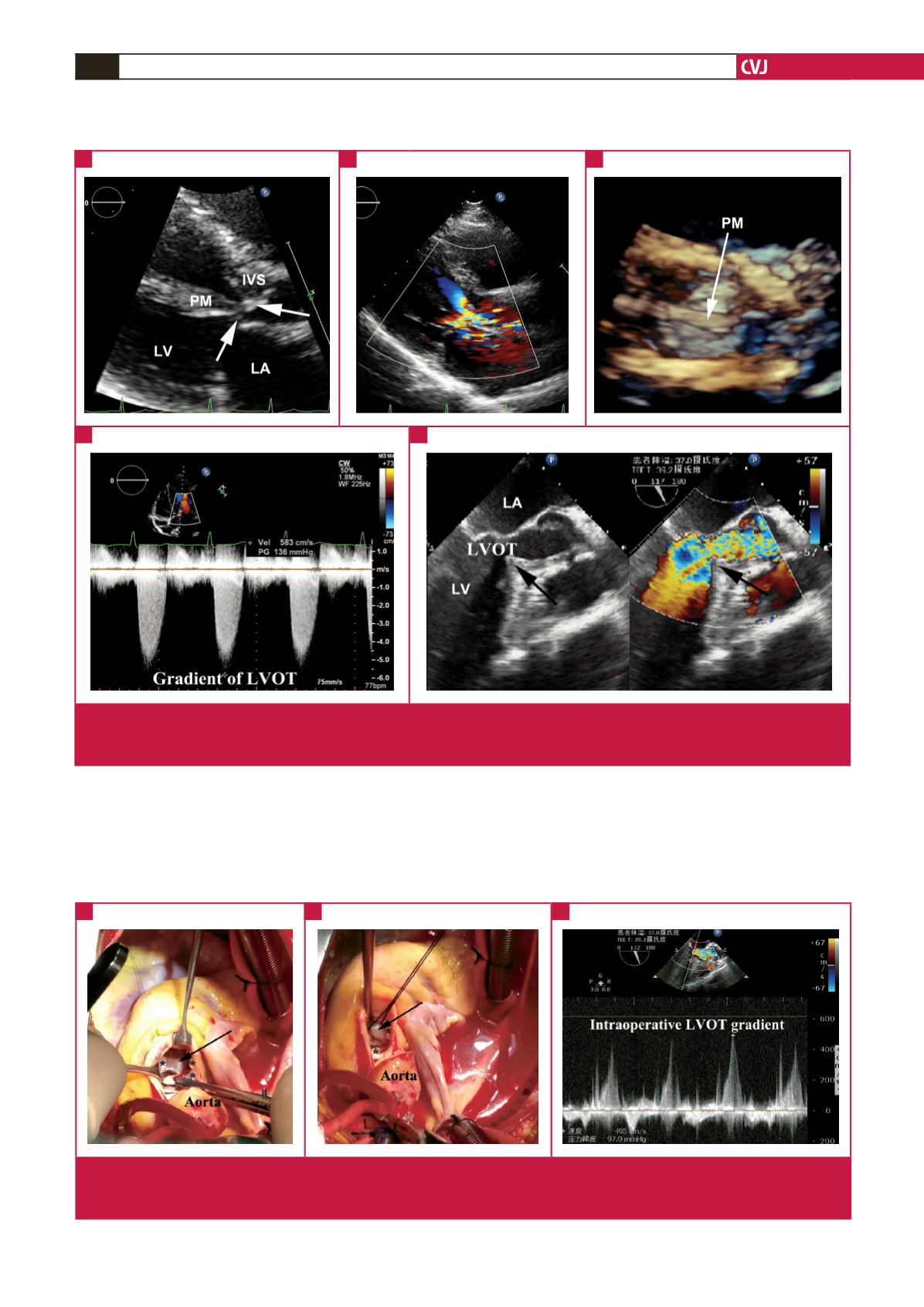
Fig. 1.
LVOT obstruction due to basal IVS hypertrophy (A) and PM malposition (A, C). B shows the narrowed blood flow of the LVOT.
Pulsed Doppler demonstrated a gradient of 136 mmHg (D). Intra-operative transoesophageal echocardiography (E) showing
the sharp angle of the IVS (black arrow).
A
D
E
B
C
Fig. 2.
The sharp angle of the basal IVS (A, black arrow) and anomalous long PM (B, black arrow) were demonstrated through a
transaortic approach (* aortic valve). After the first recovery of heart beat, transoesophageal echocardiography showed the
LVOT gradient was still about 100 mmHg (C).
A
B
C