CARDIOVASCULAR JOURNAL OF AFRICA • Vol 21, No 1, January/February 2010
34
AFRICA
seven children of mixed ethnic origin.
The primary echocardiographic findings are shown in Table
1. Tetralogy-type lesions were the most common (43%), followed
by truncus arteriosus (20%). The miscellaneous group consisted
of patent ductus arteriosus (
n
=
2), atrial septal defect (
n
=
2),
double-outlet right ventricle (
n
=
1), and mitral valve atresia with
hypoplastic left ventricle (
n
=
1). Right-sided aortic arches were
present in 17 children (43%), either as an isolated finding or in
combination with other congenital cardiac defects. Surgery was
performed in 28 patients. Full repair was possible in 16 children
and palliative procedures were carried out in 12. Low serum
calcium was observed in six patients peri-operatively. Four
patients died, one due to natural causes and three post-operative-
ly. Death occurred three months to three years after surgery.
Cleft palate was present in 32% (
n
=
14) of the patients.
Skeletal abnormalities were present in two patients, with fusion
of the radius and ulna in one patient and spina bifida in the other.
One patient had psychiatric abnormalities as well as isolated
upper motor neuron VII palsy. All children of school-going age
in our study needed either remedial classes or special schooling.
One patient was diagnosed with a T-cell deficiency and another
with hypoparathyroidism.
Anthropometric measurements were obtained in 24 (60%)
patients. Both height and weight for age were impaired compared
to normal children, as reflected by median
z
-scores of –1.8 (–4 to
0), 95% CI: –1.3 to –2.2 for height, and –2 (–4.0 to 0.7), 95% CI:
–1.4 to –2.6 for weight, respectively. Growth was analysed retro-
spectively using old records and height for age was compared
after the longest periods of follow-up (median 12.7 years, range
3.9–19.7 years). The height for age increased from a median
z
-score of –3.4 (range –1.7 to –4.5) to –2.3 (range –2.1 to –3.2),
with
p
=
0.08 and 95% CI: –1.7 to 0.2.
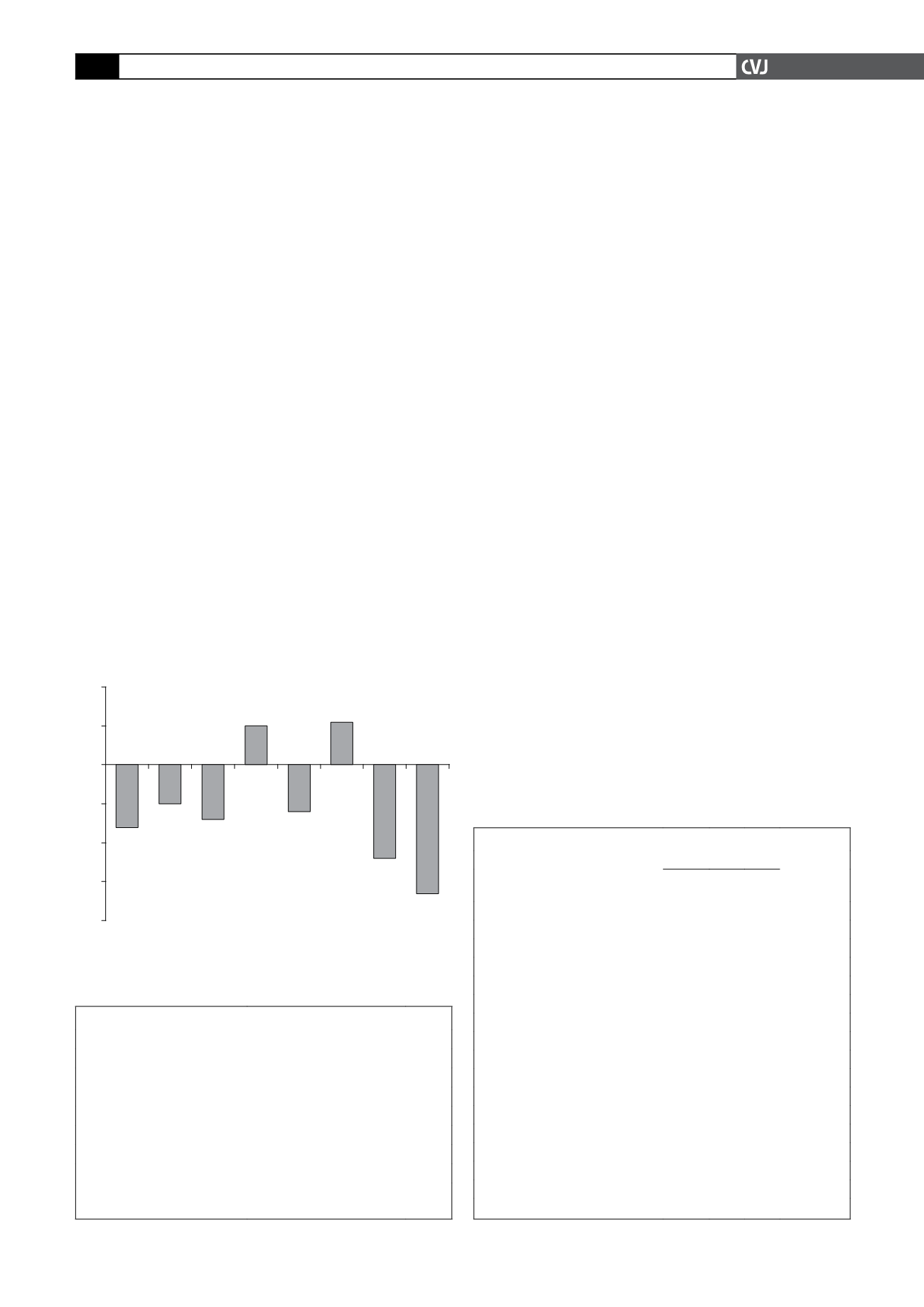
Results for individual facial measurements are shown in Table
2, while Fig. 3 shows the median
z
-values of facial measurements
differing from normal by a value of more than one. The median
z
-values for skull-base width, physiognomic height of upper face
and width of mouth tended to be smaller than normal, while the
vermilion height of the lower lip was somewhat higher than aver-
age. Both the height and width of the ears were notably smaller
than normal, with median
z
-scores of –3.3 and –2.4, respectively
(Table 1). A right-sided aortic arch was present in 52% (10/19) of
the children with a
z
-value of less than –2 for ear height (sensitiv-
ity 0.2; specificity 0.5).
Discussion
To the authors’ best knowledge, this is the first published report
on cardiac and facial features of the 22q11 microdeletion in
South African children. Our results show that microdeletions
of the long arm of chromosome 22 occur in children from the
Free State and Northern Cape provinces. Cyanotic heart lesions
were common, especially conotruncal defects. Right-sided aortic
arches were frequently found either in isolation or associated
with underlying cardiac lesions. Anthropometric abnormalities,
especially a long, narrow mid-facial area and small ears were the
most marked facial anomalies.
Cardiac abnormalities were present in 92% of our patients,
but the fact that most of these patients presented at a cardiol-
ogy unit should be taken into account. Cardiac abnormalities
are common and occur in up to 75% of children with VCFS.
9
Tetralogy of Fallot, pulmonary atresia with ventricular septal
defect (VSD) (also referred to as extreme tetralogy) and truncus
arteriosus were present in 63% of our patients. This compares
favourably with international studies where tetralogy, with or
without pulmonary atresia,
12–17
were also the most common
cardiac lesions. These are all cyanotic cardiac conditions and
TABLE 1. ECHOCARDIOGRAPHIC FINDINGS
Cardiac finding
Number of patients (
n
= 40)
%
Tetralogy of Fallot
10
25.0
PA-VSD
7
17.5
Truncus arteriosus
8
20.0
VSD
4
10.0
Isolated right-sided aortic arch
2
5.0
Normal
3
7.5
Miscellaneous*
6
15.0
PA-VSD: pulmonary atresia with ventricular septal defect; VSD:
ventricular septal defect. *See text for details.
TABLE 2.ANTHROPOMETRIC MEASUREMENTS OF THE FACE
Description
z-value
95% CI
Median
25th
%
75th
%
Skull-base width (t-t)
–1.6 –2.9 –0.5 (–2.5; –1.1)
Height of forehead (tr-n)
–1.0 –1.7 0.4 (–1.3; –0.2)
Height of mid-face (n-sto)
1.0 –0.5 3.3 (0.0; 2.5)
Width of face (zy-zy)
–1.4 –2.2 0.1 (–2.1; –0.5)
Width of mandible (go-go)
0.8 –0.6 1.9 (–2.3; 1.3)
Intercanthal width (en-en)
–0.5 –1.7 1.0 (–1.2; 0.6)
Bi-occular width (ex-ex)
–0.2 –0.9 1.9 (–2.3; 1.3)
Width of nose (al-al)
0.7 –1.2 2.0 (–0.4; 1.3)
Height of nose (n-sn)
1.0 0.0 2.6 (0.5; 2.4)
Nasal tip protrusion (sn-prn)
–0.7 –2.3 0.6 (–2.1; 0.4)
Width of columella (sn’-sn’)
0.5 –1.0 2.1 (–0.2; 1.9)
Length of ala (ac-prn)
–0.8 –2.5 0.8 (–1.9; 1.0)
Width of mouth (ch-ch)
–1.2 –2.3 –0.3 (–1.8; –0.3)
Vermilion height of lower lip (sto-li)
1.1 –0.7 2.2 (0.1; 1.6)
Width of auricle (pra-pa)*
–2.4 –3.4 –1.4 (–3.3; –1.7)
Height of ear (sa-sba)*
–3.3 –4.8 –2.6 (–4.5; –2.9)
*The width and height of ears reflects the average of both ears.
Fig. 3. Median z-values of facial measurements differing
more than one unit from normal.
2
1
0
–1
–2
–3
–4
Median z-value
Skull
base
width
Height
fore-
head
Width
mid-
face
Height
mid-
face
Width
of
mouth
Vermilion
height
lower lip
Width
ear
Height
ear
–1.6
–1
–1.4
1
–1.2
1.1
–2.4
–3.3


