CARDIOVASCULAR JOURNAL OF AFRICA • Vol 24, No 4, May 2013
AFRICA
143
used for cardiopulmonary bypass, antibiotics and catheters used
for interventional treatment are still very expensive and almost
out of reach of the poorer countries.
Table 3 gives some representative costs in Africa, India and
the United States. The International Children’s Heart Foundation
sends teams to underdeveloped countries, and cites $2 500 for
the cost of open-heart surgery; this is almost certainly subsidised.
There are additional costs to congenital heart disease beyond
surgical treatment: medical treatment, cost of transport to
hospital, which is often difficult in rural Africa andAsia, and loss
of parental working time when they have to take the children to
a medical centre.
6
These costs are disproportionately severe in
countries with low incomes per capita.
In addition, both treated and untreated children with congenital
heart disease are at risk of infective endocarditis. This risk may
differ from country to country but we do not have good data.
One current estimate by Knirsch and Nadal
7
assessed the risk
of congenital heart disease as 1.5 to six episodes per year per
100 000 adults, and 0.34–0.64 episodes per year per 100 000
children.
Infective endocarditis produces considerable morbidity,
involves lengthy and costly treatment, and severely affects
longevity.Afollow-up study of patientswith infective endocarditis
and a variety of underlying heart diseases showed that fewer than
50% survived more than 20 years after the infection.
8
Finally, children with congenital heart disease have more than
heart disease to contend with. There can be associated defects in
several other organ systems, and neurodevelopmental problems
are particularly burdensome. Marino
et
al
.
9
reported in an
American Heart Association scientific statement that moderate
to severe neurodevelopmental disabilities occurred in over 50%
of children with severe congenital heart disease or congenital
heart disease palliated as neonates, and in 25% of those with less
severe anomalies.
Resources
The resources to treat congenital heart disease are both inadequate
and seriously maldistributed.
10-12
The 2007–2009 World Society
for Paediatric Heart Surgery Manpower Survey
11
noted that about
75% of the world’s population have no access to cardiac surgery,
and that the distribution of cardiac surgeons was very unbalanced
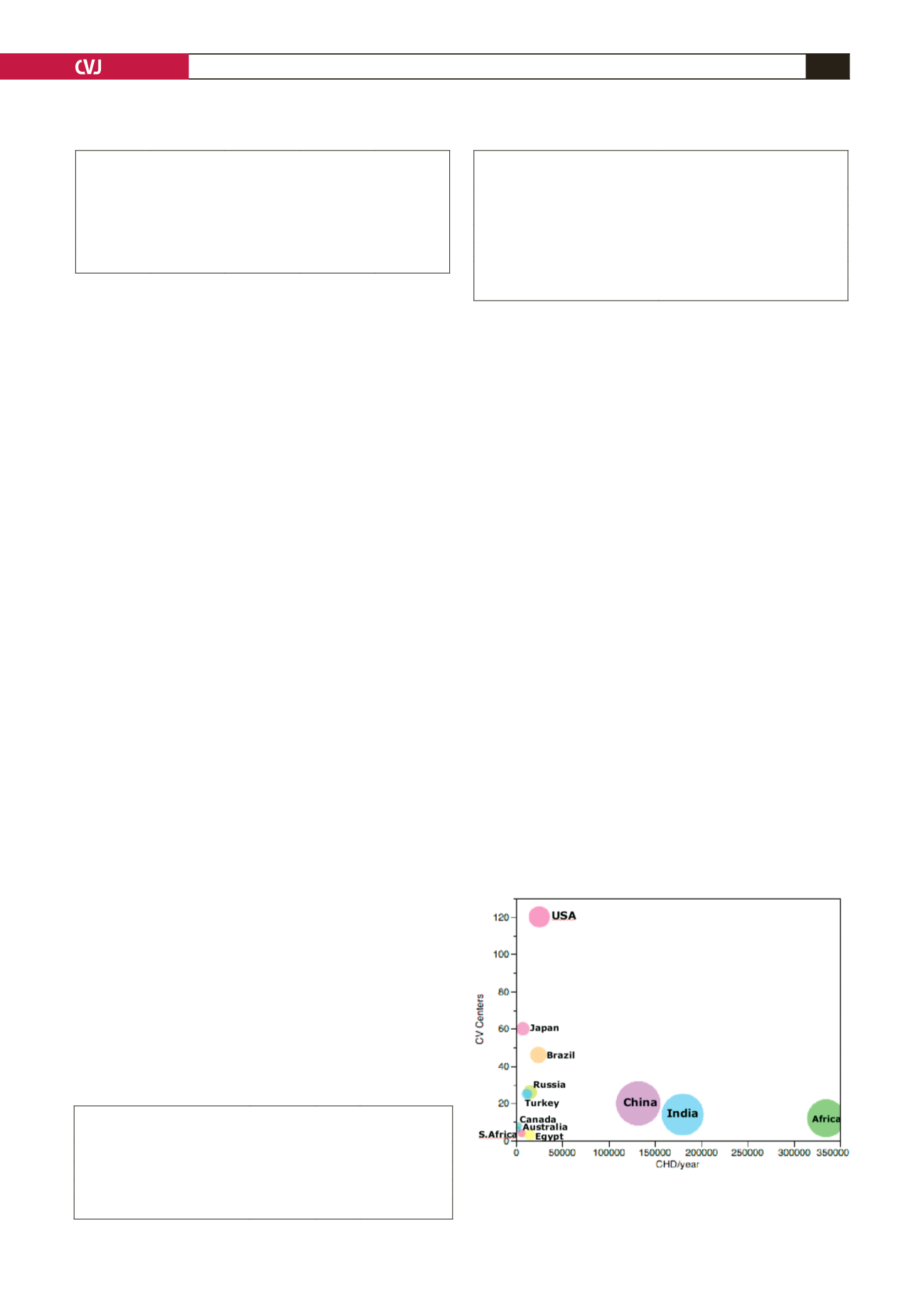
(Table 4). This is in keeping with the variation in distribution of
cardiovascular centres (Fig. 6).
Prospects and potential solutions
The issues are so complex that it is difficult to know where to
begin. Poverty, the greatest barrier to successful treatment of
congenital heart disease, has multiple causes that are complex
and difficult to remove. Natural resources may be inadequate
or, where resources (oil, diamonds, ores) exist, corrupt and
inefficient governance may prevent fair distribution. This is often
compounded by limited education of the population, including
its leaders, by unfair trade practices of the developed nations,
and at times by well-meaning but ill-advised help from outside
agencies.
13-15
In addition, in sub-Saharan Africa, there is a huge
deficit of all types of skilled medical personnel.
16
Treatment of congenital heart disease by surgery or
interventional cardiac catheterisation will always be relatively
expensive, and expense will always be a major barrier to
achieving good cardiac care of these children. This problem
is not unique to congenital heart disease, and treatment of
some non-cardiac diseases such as cancer, AIDS, drug-resistant
tuberculosis and some chronic diseases may be as expensive.
Unfortunately, attempts to alleviate poverty have had limited
success. Nevertheless there are several strategies that can help
to improve cardiac care. Because the specific problems may
differ between countries, the mix of strategies may also need to
be different.
Easing the burden of congenital heart disease can be divided
into specific cardiac approaches that can be used on a near
and mid-term time scale, and a more general socio-economic
approach that will take much longer to implement. There
are several models for the cardio-specific goals for treating
congenital heart disease in underdeveloped countries, and they
are discussed in detail by Hewitson and Zilia.
6
TABLE 2. ESTIMATES OF POTENTIAL MONEY TO SPEND ON
CHILDRENWITH CHD IN SINGAPOREAND NIGER. THE GDP
VALUESARE CORRECTED FOR LOCAL COST OF LIVING
Country
CHD/million
population
CHD/million
wage
earners
GDP per
capita
GDP/CHD
Singapore
~100
~120
$63 000
$525
Niger
~500
~850
$1 000
$0.85
TABLE 3. REPRESENTATIVE COSTS. DATA TAKEN FROM
KUMARAND BALAKRISHNAN
4
AND PASQUALI
ET AL
.
5
Service
Africa India
USA
Open-heart surgery
US$10 000 $5 000 $12 000–50 000
128-slice CT angiogram
-
$350
$4 000
Colour Doppler echocardiography $100
$30
$200
TABLE 4. RATIO OF CARDIAC SURGEONS TO POPULATION
ON DIFFERENT CONTINENTS
Continent
Ratio
cardiac
surgeons:population
North America
1:3.5 million
Europe
1:3.5 million
South America
1:6.5 million
Asia
1:25 million
Africa
1:38 million
Fig. 6. Distribution of cardiovascular centres in selected
countries and continents. The area of the bubble is
proportional to the population.


