CARDIOVASCULAR JOURNAL OF AFRICA • Vol 24, No 4, May 2013
144
AFRICA
The least appealing is to have the child and parents go where
experts can treat the child optimally. This option is available to
only a few privileged and wealthy families and does nothing to
help the majority of people in the country. A second slightly
more productive model is to have teams of doctors, nurses and
technicians go to a country for a few weeks, and treat a set
of patients who have been selected beforehand. This certainly
benefits more children, but their follow up may be inadequate,
the majority of children with congenital heart disease remain
untreated, and this model does little to improve medical services
in the country.
A better model would be to have these teams come to a
country and help train local doctors, nurses and technicians,
so that when the visitors leave, a functioning medical service
is in place locally. This course, however, involves substantial
investment by the host country that may be unwilling or unable
to maintain this degree of sophisticated medical care. Developing
locally low-cost substitutes for expensive imported products may
reduce some of this disadvantage.
For long-term socio-economic goals, larger issues than
treatment of congenital heart disease come into play. It is far
from clear that children with congenital heart disease should
get preferential use of scarce resources. In underdeveloped
countries, congenital heart disease plays a minor role in child
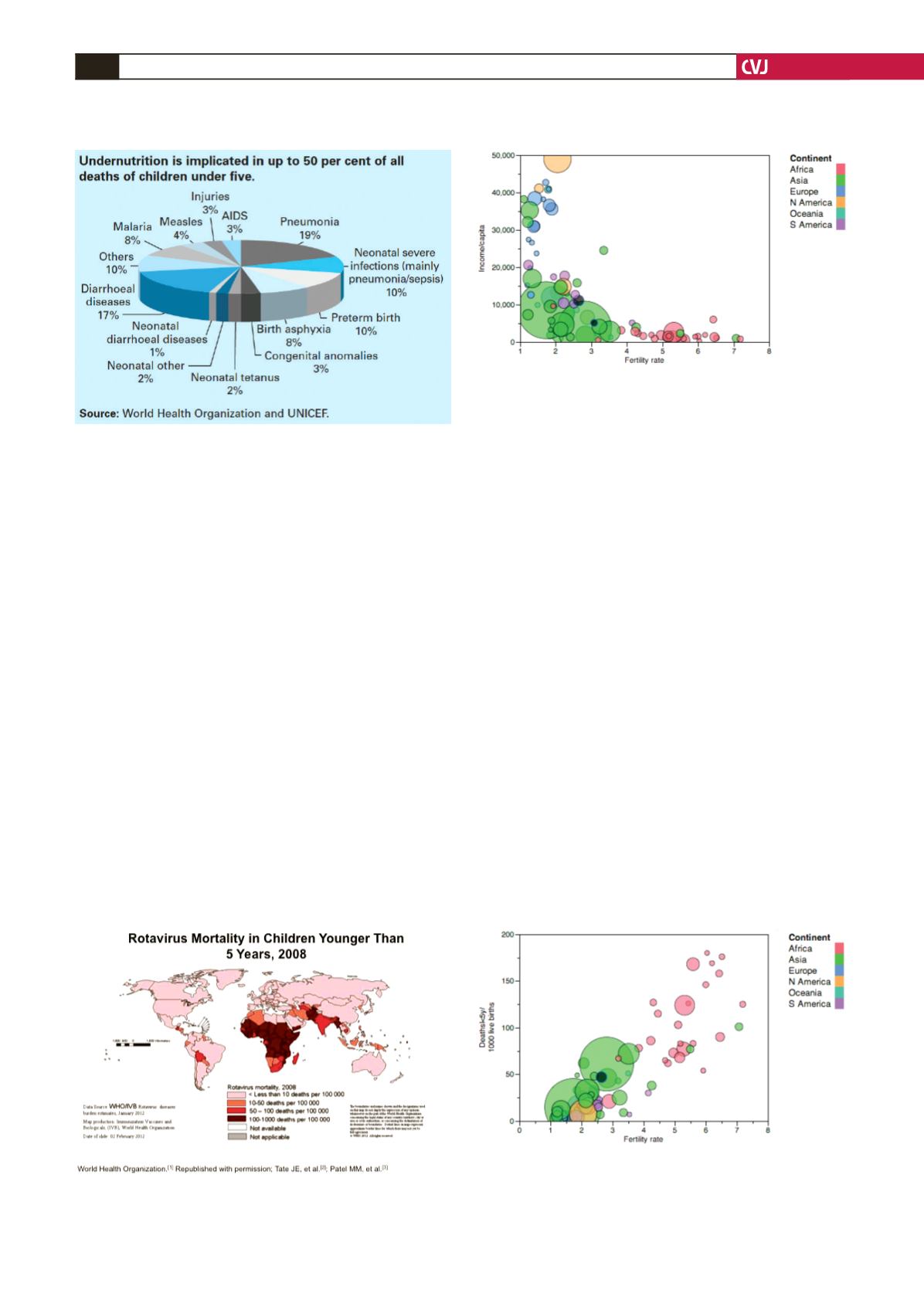
morbidity and mortality (Fig. 7).
As shown in Fig. 7, congenital anomalies of all types account
for only 5% of deaths, compared with 8% for malaria, 4% for
measles, 17% for diarrhoeal diseases, and 29% for pneumonia
and other infections, all of which are easier and cheaper to
prevent or treat than are congenital heart diseases, and would
be a better way to invest scarce resources. Fig. 8 shows, for
example, the enormous death rate from rotovirus disease, for
which an excellent and low-cost vaccine is now available but not
yet extensively used.
Finally, in this list of preventable diseases, we should mention
rheumatic heart disease. Although its prevalence is not well
defined, it probably affects as many patients as do all forms
of congenital heart disease, including bicuspid aortic valves.
Inasmuch as rheumatic heart disease usually follows repeated
episodes of acute rheumatic fever, and that treatment of acute
streptococcal pharyngitis with penicillin is cheap and effective,
this would be an excellent field into which to put scarce
resources.
6
Treating congenital heart disease, however, is always going
to be expensive, and it may be worth giving more thought to its
prevention. An approach that has been shown to be effective in
a variety of countries is to educate women and improve efforts
for family planning. The relationships between excessive fertility
Fig. 7. Causes of global mortality in children under five
years old.
Fig. 8. Distribution of rotovirus mortality across the
world. Reproduced with permission from the World
Health Organisation.
Fig. 10. Fertility rate versus deaths under five years of
age per 1 000 live births. The area of the circle is propor-
tional to the population. There is a direct relationship
between fertility rate and child mortality, with African
countries being worst off.
Fig. 9. Fertility rate versus income per capita for several
countries on different continents. The continents are
colour coded, and the area of the circles is proportional
to each country’s population. Note that countries in
Africa with high fertility rates are at the lowest end of the
income scale.


