CARDIOVASCULAR JOURNAL OF AFRICA • Vol 24, No 5, June 2013
AFRICA
173
follow-up period of 15.5
±
6.8 months (range 6–30 months), a
relapse occurred in two patients. Severe right heart failure was
seen in three cases and one fatality was reported.
Discussion
Right-sided location during infective endocarditis is rare. It
accounts for 5–10% of cases of endocarditis, according to the
literature.
2-6
Right-sided endocarditis is most often reported in
Africa, in very few cases. For instance, Ndiaye
et al
. in Sénégal
11
and Compaoré
et al
. in Moroco
12
reported six cases each. In
South Africa, Naidoo
et al
. reported 15 cases.
13
We reported
14 cases, which represented 29.1% of all infective endocarditis
during the study period.
Right-sided endocarditis is most often described in drug
addicts and in iatrogenic infections (catheter, post-surgery)
where venous access is the point of entry for the bacteria. In fact,
about 80% of tricuspid endocarditis is found in drug addicts.
14
In our study, venous access was implicated in 85.7% of
cases. Immunosuppression, which is a risk factor for right-sided
endocarditis,
15,16
was found in three patients in our cohort. In
terms of aetiology, the microorganism most frequently isolated
was
Staphylococcus aureus.
17
The clinical feature is almost invariably represented by the
infectious syndrome. In some cases tricuspid syndrome can
be found. This is a long-term fever associated with pneumonia
(usually asymptomatic), anaemia and microscopic haematuria, as
described by Nandakumar and Raju.
18
Six cases were identified
in our series.
The main diagnostic tool in our study was echocardiography
Doppler, by highlighting vegetations on the valves. Blood
sample cultures were positive in 78.5% of cases.
Treatment of infective endocarditis is based on massive
synergic long-term antibiotic therapy. The outcome is usually
favourable.
17,19,20
The prognosis of right-sided endocarditis is
usually excellent with medical treatment.
17
Complications are
most often haemodynamic. They depend on the degree of
valvular damage but also on underlying heart disease. Two cases
of death were recorded in our study because of septic shock.
Conclusion
This study shows that right-sided endocarditis is common in our
practice. This infection is prevalent in patients with congenital
heart disease or peripartum cardiomyopathy. The entry point
for microorganisms is almost exclusively the intravenous route.
Blood cultures can in most cases identify the bacterium. These
findings require health workers to pay more attention to the
maintenance of venous access in patients receiving intravenous
treatment.
References
1.
Bayer AS, Bolger AF, Taubert KA,
et al
. Diagnosis and management
of infective endocarditis and its complications.
Circulation
1998;
98
:
2936–2948.
2.
Murdoch DR, Corey GR, Hoen B,
et al
. Clinical presentation, etiol-
ogy, and outcome of infective endocarditis in the 21st century: the
International Collaboration on Endocarditis-Prospective Cohort Study.
Arch Intern Med
2009;
169
: 463–473.
3.
Sandre RM, Shafran SD. Infective endocarditis: Review of 135 cases
over 9 years
. Clin Infect Dis
1996;
22
: 276–286.
4.
Roberts WC, Buchbinder NA. Right-sided valve endocarditis: a clin-
icopathological study of twelve necropsy patients.
Am J Med
1972;
53
: 7–19.
5.
Chan P, Ogilby JD, Segal B. Tricuspid valve endocarditis.
Am Heart J
1989;
117
: 1140–1146.
6.
Goldburgh HL, Baer S, Leiber MM. Acute bacterial endocarditis of the
tricuspid valve.
Am J Med Sci
1942;
204
: 319–324.
7.
Papapanagiotou VA, Foukarakis MG, Fotiadis JN, Matsakas EP,
Zacharoulis AA. Native tricuspid valve endocarditis in a young woman.
Postgrad Med J
1998;
74
: 637–638.
8.
Moss R, Munt B. Injection drug use and right-sided endocarditis.
Heart
2003;
89
: 577–581.
9.
Grau D, Vidal N, Faucherre V, Léglise Y, Pinzani V, Blayac JP,
et al
.
Complications infectieuses induites par le mésusage de la buprénor-
phine haut dosage (Subutex): analyse rétrospective de 42 observations.
Rev Med Interne
2010;
31
: 188–193.
10. Li JS, Sexton DJ, Mick N,
et al
. Proposed modifications to the Duke
criteria for the diagnosis of infective endocarditis.
Clin Infect Dis
2000;
30
(4): 633–638.
11. Ndiaye MB, Diao M, Pessinaba S,
et al
. Aspects épidémiologiques,
cliniques et échographiques des endocardites infectieuses du cœur droit
au Sénégal : 6 observations.
Med Trop
2011;
71
: 484–486.
12. Compaoré P. endocardite infectieuse du Coeur droit. A propos de
6 observations et revue de la littérature. Thèse méd Univ Hassan II
Casablanca 2006.
13. Naidoo DP. Right-sided endocarditis in the non-drug addict.
Postgrad
Med J
1993;
69
: 615–620.
14. Robbins MJ, Frater RW, Soeiro R,
et al
. Influence of vegetation size on
clinical outcome of rightsided infective endocarditis.
Am J Med
1986;
80
: 165–171.
15. Papapanagiotou VA, Foukarakis MG, Fotiadis JN,
et al
. Native tricus-
pid valve endocarditis in a young woman.
Postgrad Med J
1998;
74
:
637–638.
16. Naidoo DP. Right-sided endocarditis in the non-drug addict.
Postgrad
Med J
1993;
69
: 615–620.
17. Varona JF, Guerra JM. Tricuspid valve endocarditis in a nonaddicted
patient without predisposing myocardiopathy.
Rev Esp Cardiol
2004;
57
(10): 993–996.
18. Nandakumar R, Raju G. Isolated tricuspid valve endocarditis in non
addicted patients: A diagnostic challenge.
Am J Med Sci
1997;
314
:
207–212.
19. Rouveix E, Witchitz S, Bouvet E,
et al
. Tricuspid infective endocarditis:
56 cases.
Eur Heart J
1984;
5
(suppl C): 111–115.
20. Chan P, Ogilby JD, Segal B. Tricuspid valve endocarditis.
Am Heart J
1989;
117
: 1140–1146.
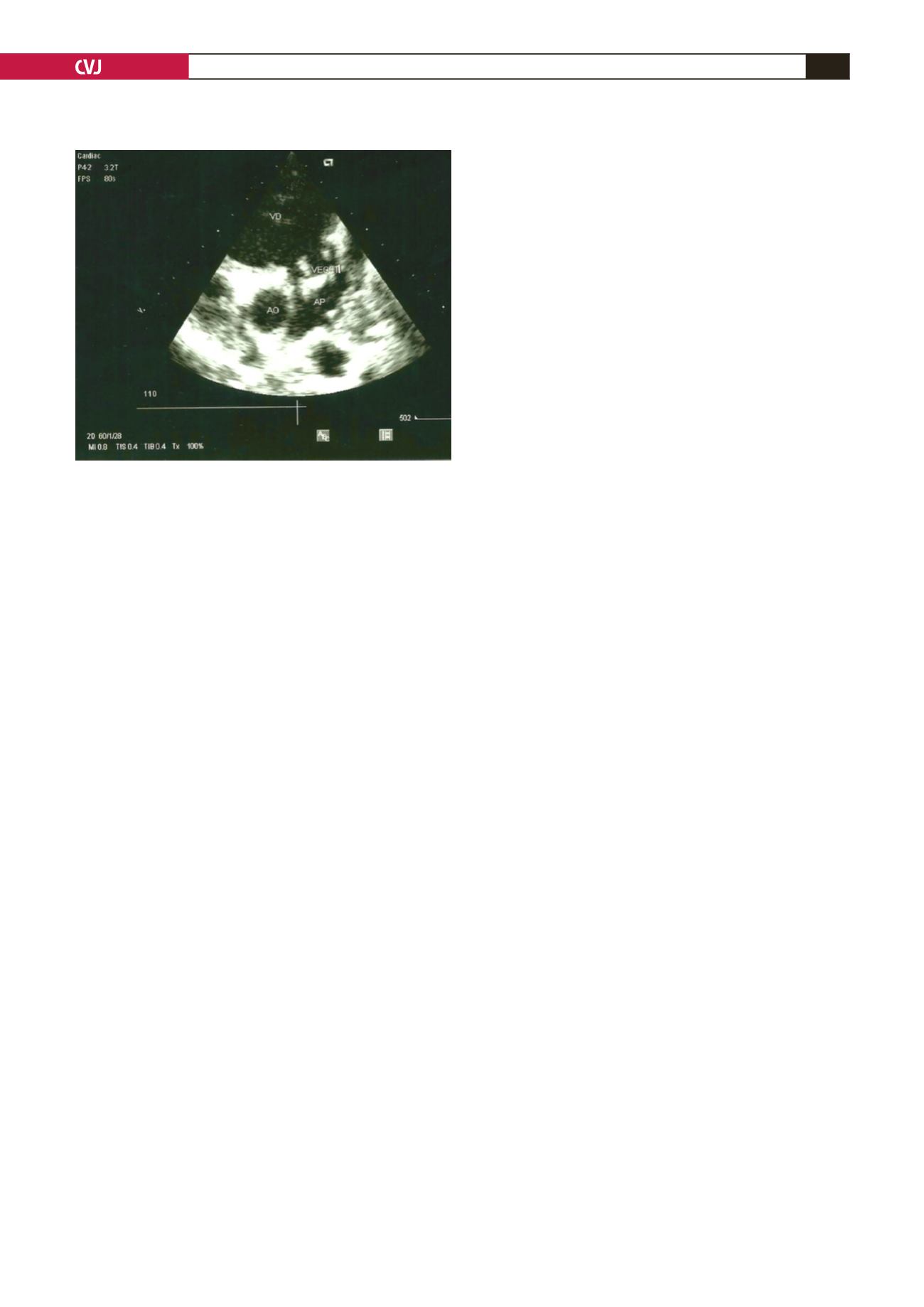
Fig. 3. Two-dimensional echocardiography, parasternal
short-axis view showing vegetations on the pulmonary
valves and pulmonary artery trunk.


