
















 61 / 92
61 / 92

CARDIOVASCULAR JOURNAL OF AFRICA • Volume 27, No 4, July/August 2016
AFRICA
263
activity questionnaires with the assistance of trained African
field workers from the communities. Before measurements
commenced, all procedures were explained to the participants
in their home language. The participants then gave written
informed consent.
Height (Invicta stadiometer IP 1465, Leicester, UK), weight
(Precision health scale, A&DCompany, Tokyo, Japan) and waist
circumference (WC) (Holtain unstretchable metal tape, Apex
Tool Group, Apex, USA) were measured using standardised
methods and calibrated instruments.
16
Body mass index (BMI)
was calculated with the formula: weight (kg)/height (m
2
).
The validated OMRON HEM-757 (Omron Healthcare,
Kyoto, Japan) device was used to measure blood pressure.
Each participant was fitted with the correct cuff size. During
the measurements, the participant was seated in a relaxed
upright position with legs uncrossed. After a resting period of
10 minutes, the brachial systolic (bSBP) and diastolic blood
pressure (bDBP) were measured on the right upper arm,
followed by a five-minute resting period and a second blood
pressure measurement. The value of the second measurement
was used for analysis. Participants were classified as hypertensive
or normotensive according to standard guidelines.
17
The cSBP was measured with the OMRON 9000AI device
(Omron Healthcare, Kyoto, Japan), which uses the second
systolic peak (reflected wave) as basis for the calculation of
cSBP. Diastolic blood pressure is assumed to be consistent
throughout the body, therefore the central pulse pressure (cPP)
was calculated by subtracting the bDBP from the cSBP.
18,19
Pulse-wave velocity (PWV) was measured non-invasively
on the left side of each participant while in a supine position.
The Complior SP device (Artech-Medical, Pantin, France)
uses superficial pulses over the carotid dorsalis pedis (cdPWV)
section of the arterial tree to estimate PWV.
The carotid characteristics were measured non-invasively
using B-mode ultrasonography with the SonoSite Micromaxx
system (SonoSite, Inc., Bothel, WA, USA), using a six- to
13-MHz linear array transducer. A minimum of two optimal
angles were used from images of the right and left common
carotid arteries. These images were then measured by a single
reader according to protocols, and digitised and imported into
the automated software of the Artery Measurements System
(Gothenburg, Sweden).
The carotid intima–media thickness (IMT) was analysed by
a single reader on a good-quality image of a maximum 10-mm
segment. The borders of the inner diameter of the blood vessel
and the near and far wall of the intima–media were identified by
an automated function of the program, but user intervention was
possible. Approximately 100 discrete measurement points within
a 10-mm segment of the carotid artery were used to obtain the
mean IMT and the carotid diameter for each participant.
The carotid cross-sectional wall area (CSWA) was calculated
according to the following formula:
CSWA
=
[3.14
×
(
LD
___
2
+
IMTf)
×
(
LD
___
2
+
IMTf)] – [3.14
×
(
LD
___
2
)
×
(
LD
___
2
)]
where LD
=
lumen diameter and IMTf
=
carotid intima–media
thickness of the far wall.
A single reader analysed video-clips of the carotid artery in
order to determine the maximum and minimum lumen diameters
(LD). The carotid distensibility (CD) coefficient was calculated
according to the following formula:
CD
=
[(2
×
delta LD
×
min LD)
+
(delta LD)
2
)
_______________________________
(cPP
×
min LD
2
]
where LD
=
lumen diameter, delta LD
=
maximum LD –
minimum LD, min LD
=
minimum LD, cPP
=
central pulse
pressure.
20
Young’s elastic modulus was calculated according to the
following formula:
Young’s elastic modulus
=
min LD
_________________
(IMT
×
distensibility)
where IMT
=
carotid intima–media thickness, min LD
=
minimum lumen diameter.
21
The beta-stiffness index was calculated according to the
following formula:
Beta-stiffness index
=
ln (cSBP/dDBP)
______________
delta LD/min LD
where delta LD
=
maximum LD – minimum LD, min LD
=
minimum LD.
22
Participants were required to fast for at least eight hours and
blood samples were taken from the ante-brachial vein with a
sterile winged infusion set and syringes. The preparation of the
serum and plasma was done according to standardised methods,
snap frozen on dry ice and stored in the laboratory at –80°C. In
the case of blood collection in a rural area, serum and plasma
were snap frozen and stored at –20°C for not more than five days.
The serum was then transported to the laboratory and stored at
–80°C for further analysis.
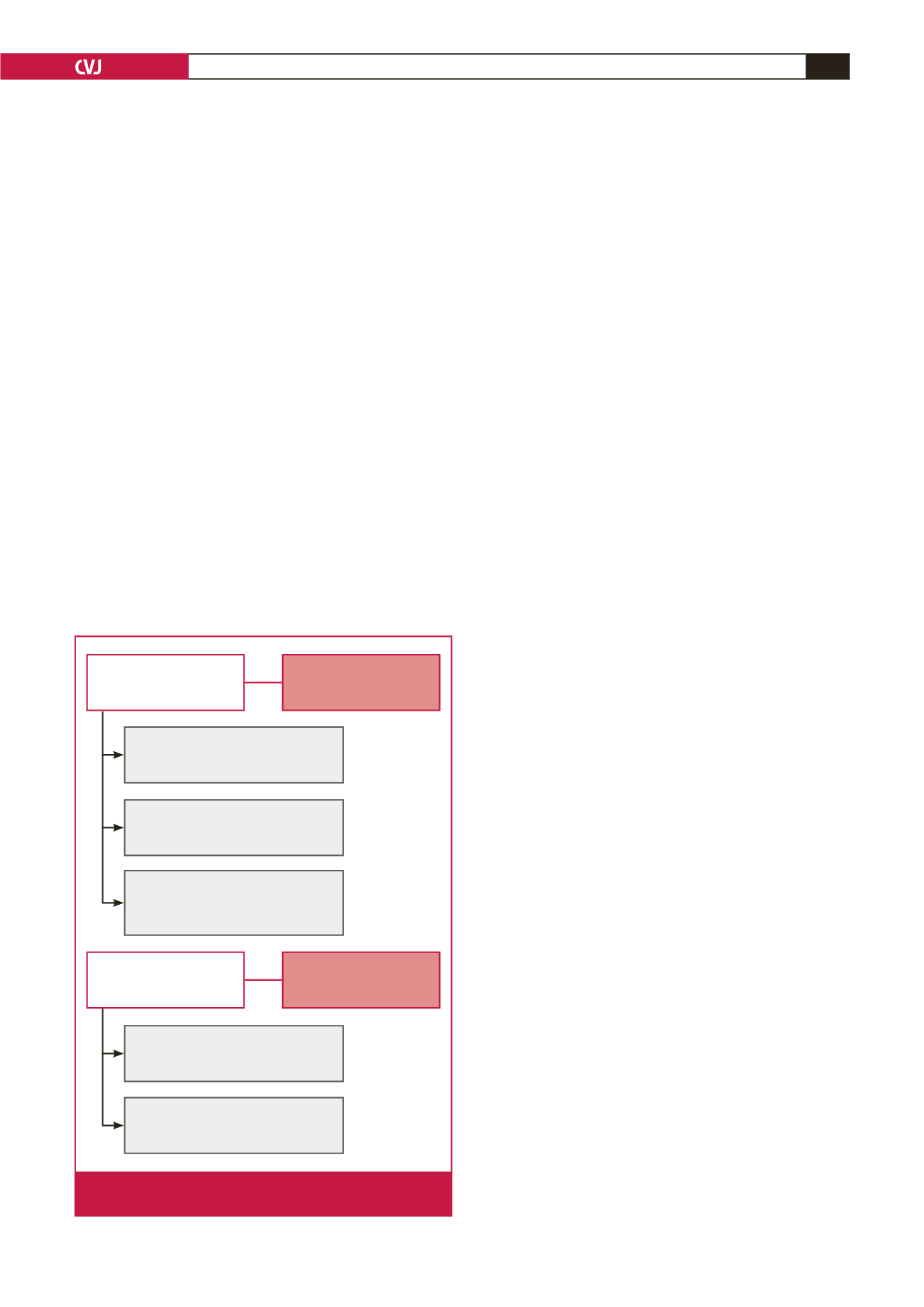
Normotensive participants
2005
(
n
=
520)
Remained normotensive
2005–2010
(
n
=
241)
Sustained hypertensive
2005–2010
(
n
=
351)
Hypertensive participants
2005
(
n
=
541)
Excluded hypertensive participants
2010
(
n
=
191)
Excluded normotensive participants
2010
(
n
=
170)
Excluded missing BP data
2010
(
n
=
20)
Excluded missing BP data
2010
(
n
=
18)
Excluded medication use (statins,
anti-inflammatory, anti-hypertensive)
2010
(
n
=
70)
Fig. 1.
Study population; all participants were HIV-free. BP,
blood pressure.