
















 78 / 92
78 / 92

CARDIOVASCULAR JOURNAL OF AFRICA • Volume 27, No 4, July/August 2016
e8
AFRICA
occur equally among men and women. The cysts range in size
from 2–3 cm, up to a maximum of 28 cm reported by Braude
et al.
8
In our case, the pericardial cyst measured 27
×
5
×
2 cm.
Most of these cases, including ours, are asymptomatic and are
diagnosed incidentally on chest X-ray.
4
The absence of symptoms
at diagnosis is a good prognostic sign. However, patients may be
admitted to a hospital with symptoms of chest discomfort or pain,
cough, dyspnoea, or palpitation due to compression of the heart.
9,10
Life-threatening complications, including cardiac tamponade,
obstruction of the right main stem bronchus, cyst infection
with cardiac or large vessel erosion and sudden death may be
encountered. Cardiac tamponade generally occurs due to intra-
pericardial rupture of the cyst. Spontaneous cyst rupture and
significant haemorrhage into the cysts have been reported, but
these have not been linked adversely to cyst size. Asymptomatic
cysts of this size are an unusual phenomenon.
11
Other reported
complications include right ventricular outflow tract obstruction,
pulmonary stenosis, atrial fibrillation, congestive heart failure,
and even sudden death after a stress test.
12-14
Pericardial cysts usually follow a benign course in the majority
of cases. There are no reports of malignant transformation.
For asymptomatic patients, conservative management with
short follow-up periods is recommended.
15
Treatment is needed
when symptoms or complications occur, and the management
of those patients should be performed in the light of clinical
characteristics. Indications for surgical resection of pericardial
cysts include large size, symptoms, cyst infection, patient request,
suspected malignancy, and prevention of complications.
10,14,16
Other treatment options for pericardial cysts include simple
observation, excision by thoracotomy, thoracoscopic surgical
removal, and percutaneous aspiration with injection of a
sclerosing agent. Although our patient was asymptomatic,
surgical excision was planned due to the large size of the cyst
and the concern that the mass was connected to the right atrium.
Conclusion
Conservative management with short follow-up periods is
recommended for asymptomatic patients with pericardial cysts.
However, surgery should be considered for patients who become
symptomatic and there is doubt about the paracardiac mass.
Our patient was unusual because of a rare giant pericardial cyst
mimicking a paracardiac mass.
This article was presented at the 10th International Congress: Update in
Cardiology and Cardiovascular Surgery (UCCVS) in March 2014.
References
1.
Losanoff JE, Richman BW, Curtis JJ, Jones JW. Cystic lesions of the
pericardium. Review of the literature and classification.
J Cardiovasc
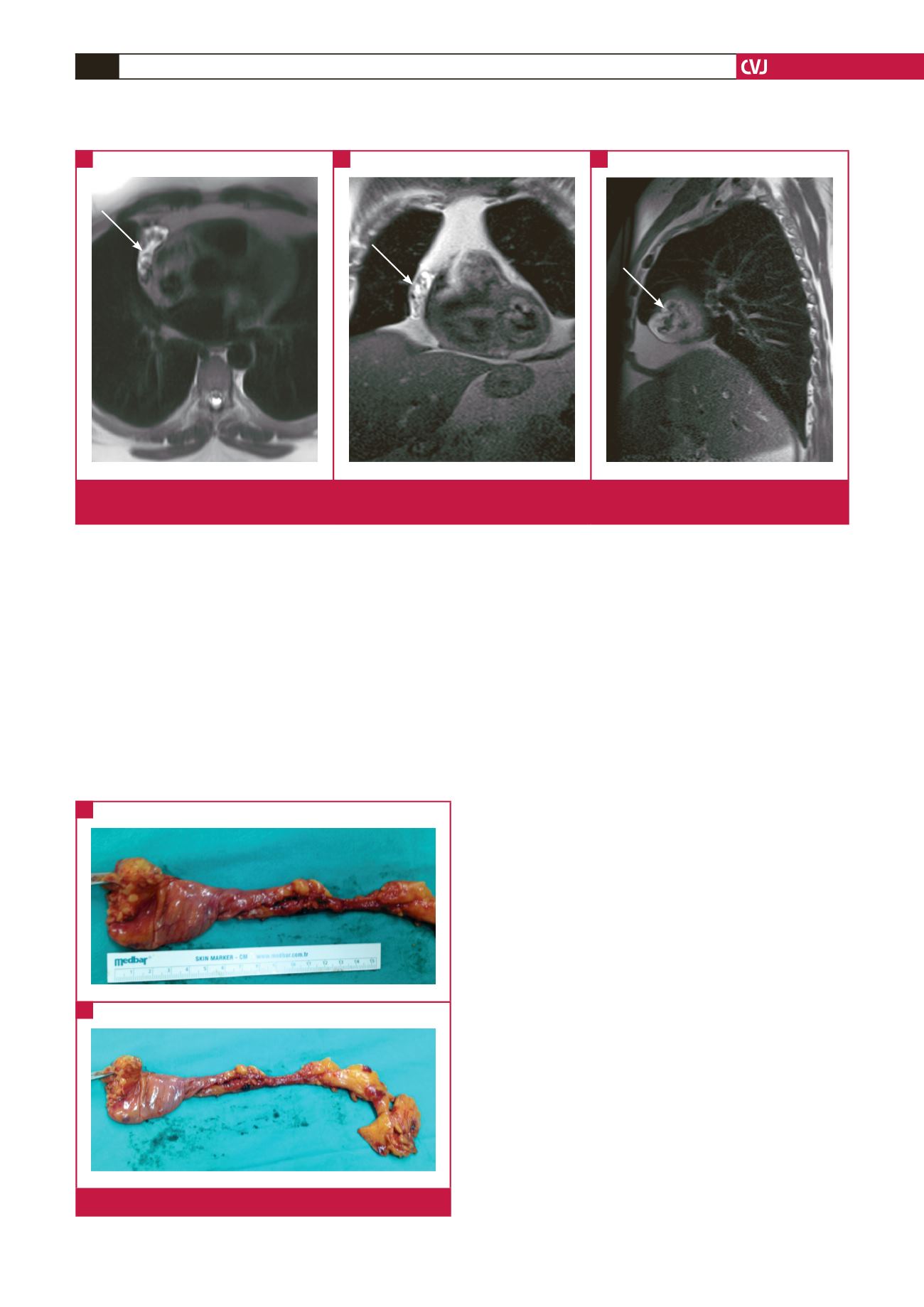
Fig. 2.
Image of the excised cystic mass.
A
B
Fig. 1.
Axial (A), coronal (B) and sagittal (C) views of T2-weighted images in the paracardiac area showing a heterogeneous hyper-
intense mass (arrows).
A
B
C