
















 55 / 88
55 / 88

CARDIOVASCULAR JOURNAL OF AFRICA • Volume 28, No 4, July/August 2017
AFRICA
257
Reviewing the causes of electrocardiographic pauses
Charle Viljoen, Robert Smith, Ashley Chin
Abstract
The electrocardiographic term ‘pause’ refers to the prolonged
R-R interval that represents the interruption in ventricular
depolarisation. This article presents a case of sinus node
dysfunction and provides a diagnostic approach to pauses on
the ECG.
Keywords:
ECG, sinus node dysfunction, SA exit block, sinus
arrest
Cardiovasc J Afr
2017;
28
: 257–260
www.cvja.co.zaDOI: 10.5830/CVJA-2017-041
A 48-year-old man was referred to the Cardiac Clinic at Groote
Schuur Hospital for evaluation of suspected symptomatic aortic
stenosis. He had a medical history of hypertension, which was
well controlled on amlodipine 10 mg and atenolol 50 mg once
daily.
He had presented with three episodes of syncope in the
three months prior to assessment. The syncope was not related
to exertion, standing or other specific situations and occurred
without any prodrome. He was not troubled by any dyspnoea,
and he denied chest pain and any palpitations.
Examination excluded severe aortic stenosis. He had regular,
good volume pulses, a normal jugular venous pressure and
an undisplaced apex beat with normal character. There was
a soft ejection systolic murmur, best heard at the lower left
sternal border with no radiation. The lung bases were clear.
An electrocardiogram (ECG) and echocardiography were
performed. Echocardiography showed a normal aortic valve
with no evidence of aortic stenosis.
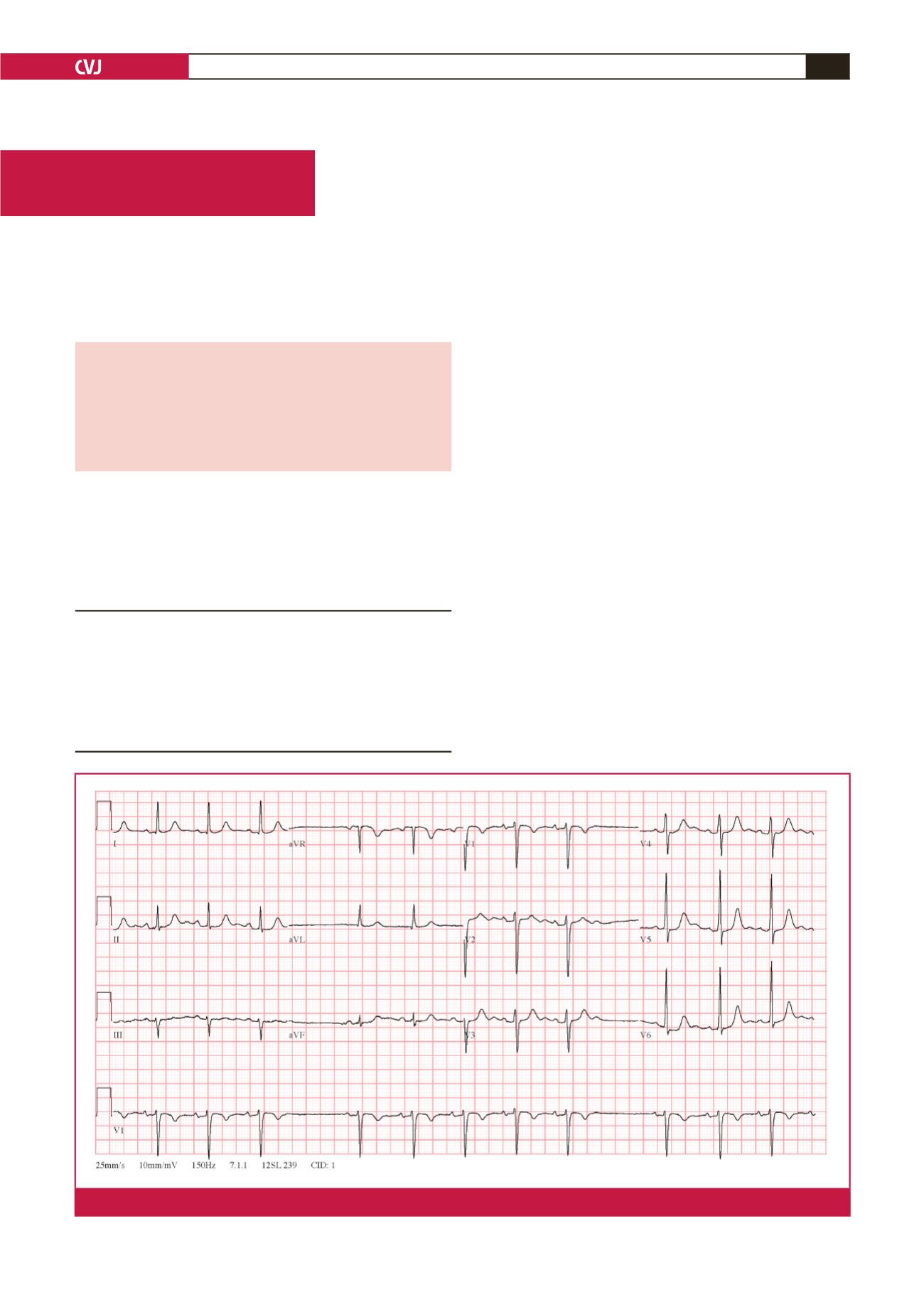
TheECG(Fig. 1) showed an irregular rhythmwith intermittent
pauses. There were no premature complexes preceding the
pauses. However, during each of the pauses, there were no P
waves at the expected time interval. The R-R interval during
the pause was twice the R-R interval before and after the pause.
Division of Cardiology, Groote Schuur Hospital and the
University of Cape Town, South Africa
Charle Viljoen, MB ChB, MMed, FCP (SA),
charleviljoen@gmail.comAshley Chin, MB ChB, FCP (SA), MPhil
Department of Medicine, Groote Schuur Hospital and the
University of Cape Town, South Africa
Robert Smith, MB ChB
ECG Series
Fig. 1.
The 12-lead ECG is in keeping with sino-atrial exit block.