


















 39 / 64
39 / 64

CARDIOVASCULAR JOURNAL OF AFRICA • Volume 31, No 5, September/October 2020
AFRICA
259
in 24/50 (48%), moderate in 10/50 (20%), large in 4/50 (8%) and
not recorded in 12/50 (24%).
Of 31 patent ductus arteriosus (PDA) lesions, the size was
small in 12 (38%), moderate in four (13%), large in 10 (32%) and
not recorded in five (16%).
Gender and age differences between the most common
congenital and acquired cardiac lesions are compared in Table
3. There was a slight male predominance in children with atrio-
ventricular septal defect (AVSD) (58%) and cor pulmonale
(80%). The median age of children with CHD was lower than
children with an acquired cardiac lesion (0.9 vs 3.2 years;
p
=
0.001 by two-sample Wilcoxon rank-sum). Among CHD lesions,
patients with TOF had the highest median age (5.4 years),
whereas all other patients with CHD lesions had a median age
of 2.4 years or younger.
From 2010 to 2012, 170 patients with CHD were seen at the
PMH cardiac clinic, equating to 57 per year. As 57 CHD cases
per year reflects only the echocardiography reports of one of
two paediatric cardiologists, we doubled this number to estimate
the real number seen by two paediatric cardiologists (114 in one
year). Using Botswana’s 2012 annual birth cohort of 40 856 from
the Botswana Vital Statistics Report, the estimated prevalence of
CHD was 114/40 856
=
2.8/1 000 live births.
For the comparator group in the three months of 2014,
99/172 patients seen at PMH cardiac clinic had CHD. This was
an estimate of 198 cases seen in one year. Using Botswana’s 2012
annual birth cohort of 40 856 (as numbers were not available for
2014), the estimated prevalence of CHD was 198/40 856
=
4.95/
1 000 live births.
Discussion
This is the first study exploring the clinical spectrum and
prevalence of CHD in children in Botswana. The project focused
on PMH, the referral site for paediatric cardiology for the
country. The estimated prevalence of CHD was between 2.8 and
4.95/1 000 live births.
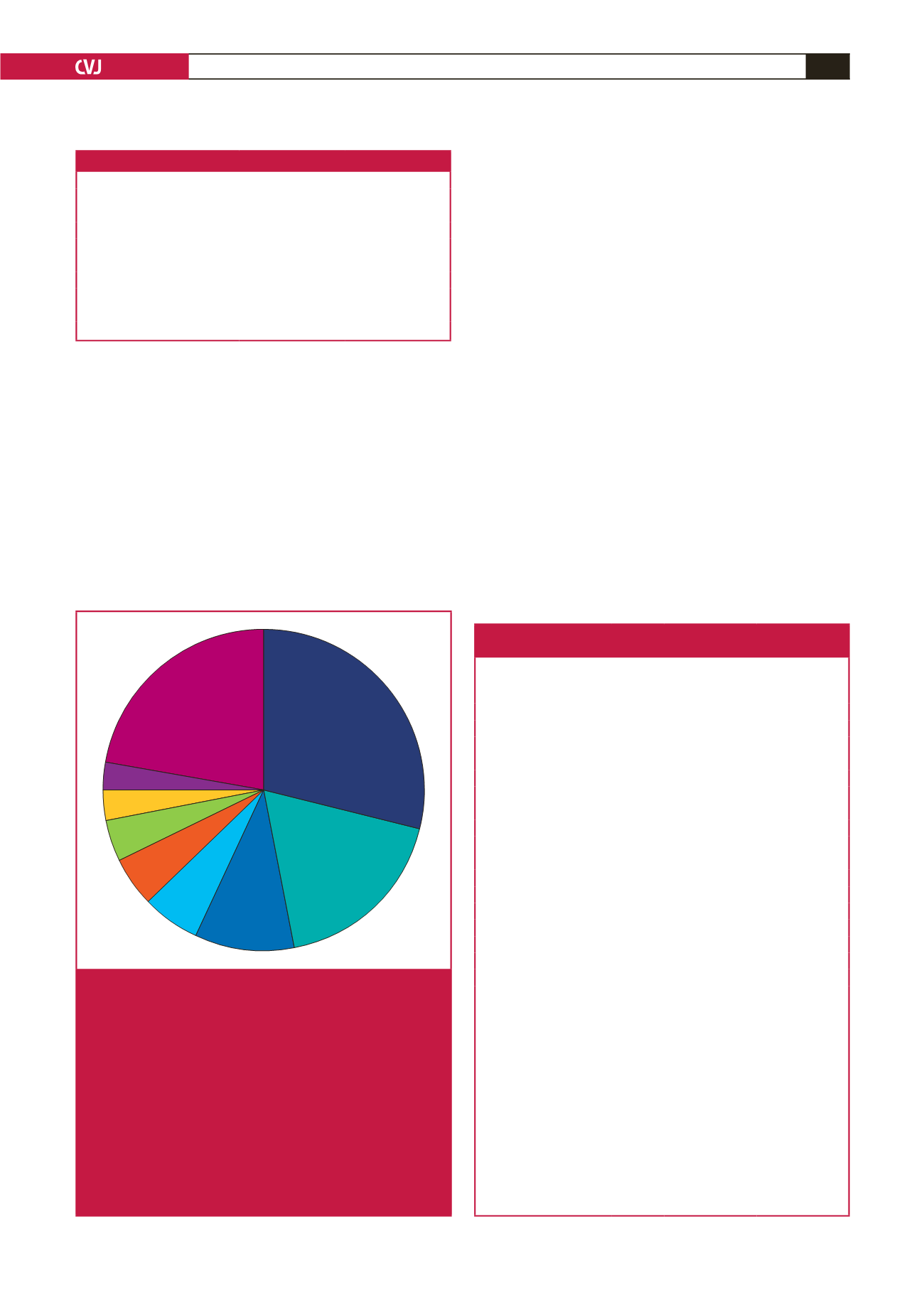
PDA & VSD
4%
PDA
18%
AVSD
10%
TOF
6%
PS
5%
VSD
29%
Other
22%
ASD
3%
TA
3%
Fig. 2.
Pie chart showing the distribution of CHD by pathology
for the study group (
n
=
170).
Note:
other
includes four (2%) each of AR; three (2%) each
of DORV (with PS), D-TGA, HLHS; two (1%) each of L-TGA,
TR, CHD
>
two lesions; and one (0.6%) each of PAPVD, PS
(with intra-cardiac shunt), AS, CoA (with VSD), MS, DORV
(without PS), TAPVR, truncus arteriosus, single ventricle,
primary pulmonary hypertension, mitral insufficiency, PR,
PDA + ASD, and shone complex.
ASD, atrial septal defect; AVSD, atrioventricular septal defect;
PDA, patent ductus arteriosus; PS, pulmonary stenosis; TA,
tricuspid atresia; TOF, tetralogy of Fallot; VSD, ventricular
septal defect.
Table 2. Indications for echocardiography
Indication
Number (n
=
377)
Percentage*
Risk factors for CHD
95
25
Suspected CHD
75
20
Follow up
66
17
Murmur
59
16
Post-operative
35
9
Cardiomegaly
32
8
Heart failure
7
2
Unknown
8
2
*Total approximated percentages
=
99% due to rounding.
Table 3. Distribution of congenital and acquired
heart disease according to gender and age
Cardiac lesion
Number
(%)
Boys
(% found in boys)
Age (years)
Median (Q1, Q3)
Congenital
n
=
170
n
=
85
VSD
50 (29)
24 (48)
1.9 (0.2–5.1)
PDA
31 (18)
13 (42)
0.2 (0.1–0.7)
AVSD
17 (10)
10 (58)
0.4 (0.1–0.8)
TOF
11 (6)
6 (54)
5.4 (1.6–11.3)
PS
9 (5)
5 (55)
2.2 (0.6–4.7)
VSD + PDA
6 (4)
3 (50)
0.4 (0.2–0.9)
TA
5 (3)
2 (40)
0.9 (0.5–1.8)
ASD*
5 (3)
2 (40)
0.3 (0.1–0.5)
Others
#
36 (21)
20 (56)
3.3 (0.1–5.8)
Total
170
85 (50)
0.9 (0.2–4.1)
Acquired
n
=
57
n
=
29
Cardiomyopathy
22 (39)
9 (41)
5.4 (0.9–10.8)
Pericardial effusion
17 (29)
8 (47)
1.4 (0.6–5.3)
Cor pulmonale
10 (17)
8 (80)
3.5 (1.4–7.1)
Rheumatic heart disease
7 (12)
3 (42)
11.0 (5.2–14.5)
Malignancy
1 (2)
1 (100)
0.1 (0.1–0.1)
Total
57
29 (51%)
3.2 (1.2–10.8)
SD, standard deviation; Q1, 1st quartile; Q3, 3rd quartile.
*ASD includes ostium secundum and ostium primum.
#
Other congenital heart disease includes: DORV (four), AR (four), D-TGA
(three), HLHS (three), L-TGA (two), TR (three), CHD
>
two lesions (two),
mitral insufficiency (two), PAPVD (one), PS with intracardiac shunt (one), AS
(one), Ao co-arctation (one), MS (one), TAPVR (one), truncus arteriosus (one),
single ventricle (one), primary pulmonary hypertension (one), PR (one), PDA
+ASD (one), Shone complex (one), VSD +ASD (not AV canal) (one), aortic
root dilatation (one).
AR, aortic regurgitation; AS, aortic stenosis; ASD, atrial septal defect; AVSD,
atrio-ventricular septal defect; CoA, co-arctation of the aorta; DORV, double-
outlet right ventricle; HLHS, hypoplastic left heart syndrome; MS, mitral
stenosis; PAPVD, partial anomalous pulmonary venous drainage; PDA, patent
ductus arteriosus; PR, pulmonary regurgitation; PS, pulmonary stenosis; TA,
tricuspid atresia; TAPVR, total anomalous pulmonary venous return; L-TGA,
levo-transposition of the great arteries; D-TGA, dextro-transposition of the
great arteries; TOF, tetralogy of Fallot; TR, tricuspid regurgitation; VSD,
ventricular septal defect.