


















 39 / 61
39 / 61

CARDIOVASCULAR JOURNAL OF AFRICA • Volume 32, No 4, July/August 2021
AFRICA
211
changes. The biggest impact of the BMI adjustment was on
the intercepts, shifting each BP’s mean trajectory downwards
(116.2 to 105.0 mmHg for SBP, and 75.7 to 63.3 mmHg for
DBP). Model 2, as shown in Table 4, includes a random effect
in the baseline values (intercept) to address the variability in
starting point for each individual in the sample. Model 3 in
addition to model 2, allowed a random BMI effect (slope) for
each individual to explain variability in the slope (change by
BMI).
The estimated SBP and DBP for the whole sample at 22
years of age was 105.0 and 63.3 mmHg, respectively, and each
individual value varied randomly around these baseline values
with 24.3 mmHg standard deviations for SBP and 17.5 mmHg
for DBP. Therefore 95% of the estimated individual’s BPs at age
22 years lies between 105.0 ± 1.96 × 24.3 = (57.4–152.6) for SBP
and 63.3 ± 1.96 × 17.5 = (29.0–96.7) for DBP. The estimated
increases in BP for every 1 kg/m
2
increase in BMI are 0.41
mmHg for SBP and 0.46 mmHg for DBP for the total sample.
But the individual slopes (BMI effect) vary randomly around
these values with standard deviations of 0.65 mmHg for SBP
and 0.52 mmHg for DBP. Therefore the 95% CI for BMI slopes
lie between 0.41 ± 1.96 × 0.65 = (–0.86–1.68) for SBP and 0.46 ±
1.96 × 0.52 = (–0.56–1.48) for DBP.
The correlation between the random intercepts and BMI
random slopes is strongly inversely proportional (–0.82 for SBP
and –0.87 for DBP) implying that higher values of baseline BP
at the individual level were associated with a relatively smaller
effect of BMI on BP, and vice versa. By including a random
BMI effect, the ICC (correlation among observations within an
individual) increased from 0.47 (model 2) to 0.72 (model 3) for
SBP and from 0.49 to 0.79 for DBP. In addition, the variability
in the random intercepts also increased from 14.4 (model 2) to
24.3 (model 3) for SBP, and from 9.1 (model 2) to 17.5 (model
3) for DBP.
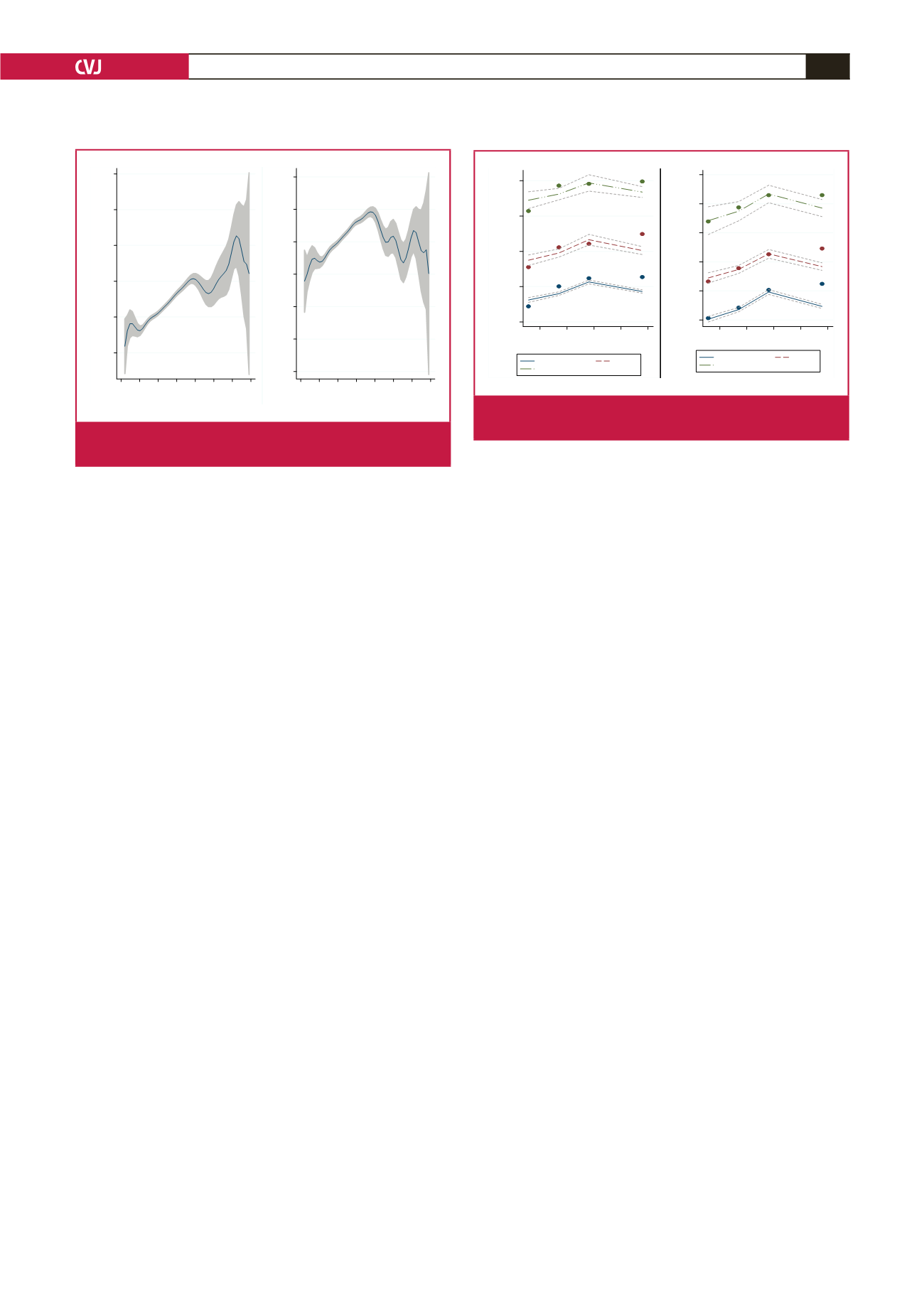
There were three distinct groups from the 1 969 individuals
(Fig. 2). The low-BP trajectory group comprised the majority
of the study participants (70.4% for SBP and 59.3% for DBP),
and showed a trajectory that was initially in the normotensive
state but gently rose to the pre-hypertensive region. A medium
BP trajectory (24.5% for SBP and 36.0% for DBP) had an initial
average BP in the pre-hypertensive state that gradually rose to
the hypertensive level, while the third group of about 5.0% had
highly elevated increasing BPs throughout. Individuals in the
medium and highly elevated BP groups were most likely to be
aged 40 years and above at baseline, while most of those in the
low-BP group were 40 years and below initially.
Discussion
This study examined BP life-course trajectories for a period
of approximately 10 years in women from an urban setting in
South Africa, and how these trajectories were related to changes
in BMI. The trajectories were initially characterised by a short
instance of decreasing SBP and DBP with age up to around
30 years (Fig. 1, Table 4). Although our sample for ages below
30 years was small, which could have affected the shape of the
trajectories, other studies have shown small downward changes
in BP in early adulthood, which could be associated with capacity
for vascular repair or adaptations.
20-22
Possible vascular repair
could be a reason for our results showing that the percentage of
subjects recovering from the hypertensive to the normotensive
state was highest (Table 3) in the relatively younger ages.
A second phase of rapid increase in the trajectories began
from around 30 up to 60 years. This closely mirrors data
from the Framingham Heart Study, which showed that SBP
increased continuously between 30 and 84 years, but for DBP the
continuous increase was between 30 and 49 years.
23
Increasing
SBP and DBP are associated with increased peripheral vascular
resistance up to around 50 years, while large arterial stiffness
leads to the steeper rise in SBP after 50 years.
24
Studies have
shown that younger women have less stiff arteries compared
with men of a similar age,
25,26
but increased stiffness occurs after
menopause. Attention for control of BP in post-menopausal
women would therefore reduce the risk for cerebrovascular and
cardiovascular events.
24
Understanding the variation in midlife
BP trajectories, and factors associated with this acceleration,
may be important in understanding the risk of development and
the prevention of CVD, and to implement strategies for lowering
BP, as per the National Strategic Plan.
8
A third phase from around 60 years of age showed a flattening
or slightly decreasing trajectory for both BPs (Fig. 1, Table 4).
Similar studies have shown a decreasing trend for SBP at ages >
65 years,
27
and for DBP from > 55 years.
28
A decline in BP in old
100
120
140
160
180
AverageSBP (mmHg)
42 44 46 48 50
Average age (years)
Low
Medium
Highlyelevated
70
80
90
100
110
120
AverageDBP (mmHg)
42 44 46 48 50
Average age (years)
Low
Medium
Highlyelevated
Fig. 2.
Observed and BMI-adjusted SBP and DBP trajecto-
ries by average age at data-collection time points.
100
120
140
160
180
200
Systolicbloodpressure (mmHg)
20 30 40 50 60 70 80 90
Age (years)
40
50
60
70
80
90
100
Diastolicbloodpressure (mmHg)
20 30 40 50 60 70 80 90
Age (years)
Fig. 1.
SBP and DBP trajectories with 95% confidence inter-
val (greyed) by age.