CARDIOVASCULAR JOURNAL OF AFRICA • Vol 23, No 4, May 2012
AFRICA
207
cardiothoracic unit of the University College Hospital, Ibadan
with a three-year history of easy fatigability, exertional dyspnoea
and weight loss. There was a history of cough productive of
whitish sputum. There was an associated history of orthopnoea,
chest discomfort and bulging chest, but no history of leg swelling.
The patient was wasted and afebrile with a respiratory rate of 32
breaths/min. Her blood pressure and pulse were, respectively,
105/80 mmHg and 102 per min. Her neck veins were distended
and she had a bulging anterior chest and hepatomegaly.
The patient’s packed cell volume was 40%. Her blood
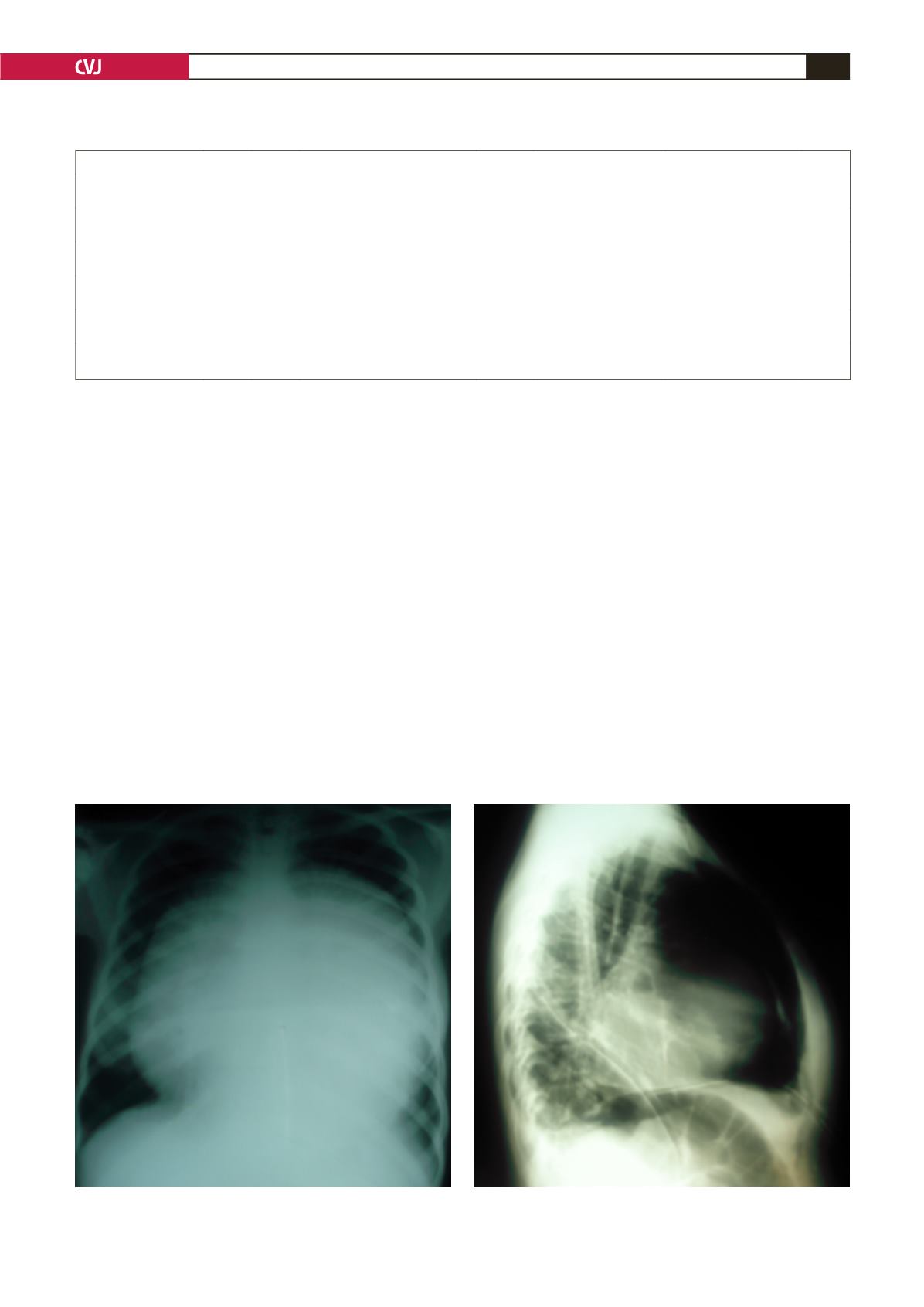
chemistry findings were normal. The chest radiograph showed
a globular heart shadow (Fig. 1). The ECG revealed low-voltage
waves. An echocardiogram revealed a large pericardial effusion
with echo speckles within it and a thickened pericardium.
There was septal bounce and a dilated inferior vena cava
with blunted respiratory fluctuations in diameter. A diagnostic
pericardiocentesis yielded serosanguinous fluid.
The patient underwent a subxiphoid tube pericardiostomy
with pericardial biopsy. A postoperative chest radiograph
showed evidence of pericardial calcification (Fig. 2). She was
scheduled for an elective pericardiectomy, which was declined.
The pericardiostomy tube was removed one week post operation.
A subsequent radiograph revealed evidence of re-accumulation
of pericardial fluid. The patient and her relatives still declined
surgery and asked for a discharge.
She represented about 48 hours later with evidence of
massive pericardial effusion and cardiac tamponade. She then
had an emergency pericardiocentesis under echocardiographic
guidance, during which 1 940 ml of haemorrhagic effusion was
aspirated and another 2 250 ml four days later. She improved
following this and then had a pericardiectomy.
Findings at surgery included a thickened parietal and visceral
pericardium, about 1.5 l of serosanguinous fluid in the pericardial
space, and an area of calcification particularly over the right
atrium (Fig. 3A, B). Both the parietal and visceral pericardium
were stripped. The patient had an uneventful postoperative
recovery period and was discharged home 10 days after surgery.
She has been seen twice since discharge, the last visit eight
months post operation, with remarkable recovery, and NYHA
class I status.
SM had a pre-operative (pericardial window) echo, which
showed effusion with constrictive physiology. He had modest
TABLE 1. SUMMARY OF CASES OF EFFUSIVE–CONSTRICTIVE PERICARDITIS
Patient
Age
(years) Gender
Comorbid conditions
HIV
status
Initial procedure
Pericardial histology
Post-op
NYHA
1. SB
Pre-op NYHA III
46
M Superficial thigh wound from
gunshot
Negative Pericardial window and
biopsy
Tuberculous pericarditis II
2. DS
Pre-op NYHA III
19
M
Haemoglobin AS
– Pericardial window and
biopsy
Non-specific calcific
pericarditis
I
3. AO
Pre-op NYHA IV
20
F
–
Negative Pericardial window and
biopsy
Non-specific chronic
pericarditis
I
4. MN
Pre-op NYHA IV
19
F
Endomyocardial fibrosis
Tricuspid regurgitation
Negative Pericardial window and
biopsy
Pericardial fibrosis
I
5. OS
Pre-op NYHA IV
20
M Fournier’s gangrene
Upper gastrointestinal bleeding
Negative
Pericardial window
Non-specific chronic
pericarditis
I
Fig. 1. Radiograph showing massive globular heart
shadow.
Fig. 2. Radiograph showing evidence of pericardial calci-
fication.


