CARDIOVASCULAR JOURNAL OF AFRICA • Vol 23, No 4, May 2012
210
AFRICA
pericardial exudate with elevated biomarkers of tuberculous
infection, and/or appropriate response to a trial of anti-
tuberculosis chemotherapy.
The diagnostic difficulty is best demonstrated by a recent
series of patients with tuberculous pericarditis where most
patients were treated on clinical grounds, with microbiological
evidence of tuberculosis obtained in only 13 (7.0%) patients.
4
Hence, the focus currently is on indirect tests for tuberculous
infection, including ADA levels and more importantly, lysozyme
or IFN-
γ
assay, which appears to hold promise for reaching
diagnosis of cases arising secondary to tuberculosis.
14-18
Technical
and financial constraints may, however, limit the diagnostic
utility of IFN-
γ
in many developing countries.
1
These tests are
currently not available in our centre.
The importance of recognising the haemodynamic syndrome
of tamponade and constriction characteristic of effusive–
constrictive pericarditis lies in an acknowledgment of the
contribution of the visceral layer of the pericardium to the
pathogenesis of constriction and of the need to remove it surgically.
However, not only is it sometimes surgically challenging to do
an epicardectomy in some patients due to a flimsy, fibrinous
visceral pericardium with attendant risk of haemorrhage; some
patients may recover with medical treatment alone – so-called
transient effusive–constrictive pericarditis.
3,19
Three of the
patients in this series actually had intra-operative haemorrhage
from atrial or ventricular injury during the epicardectomy part
of the procedure.
Visceral pericardiectomy is therefore a much more difficult
and hazardous procedure than parietal pericardiectomy, but
it is necessary for a good clinical result in cases of effusive–
constrictive pericarditis. The clinical decision as to which
patients need to be observed on medical treatment depends on
presumed or confirmed aetiology, timing of presentation, and
response to medical therapy.
Decision based on aetiology
Causes of effusive–constrictive pericarditis are varied and
usually practice-dependent. Tuberculosis is said to be responsible
for approximately 70% of cases of large pericardial effusion and
most cases of constrictive pericarditis in developing countries.
However, in industrialised countries, tuberculosis accounts for
only 4% of cases of pericardial effusion and an even smaller
proportion of instances of constrictive pericarditis.
14
Series from
Europe and North America report a predominance of idiopathic
cases, followed by cases that occur after radiotherapy or cardiac
surgery, or as a result of neoplasia or tuberculosis.
3,11,20
The aetiological spectrum indeed reflects the general
aetiological spectrum of pericardial diseases in each area
and can be influenced by the changing aetiological spectrum
of pericarditis in general and constrictive pericarditis in
particular.
3,21,22
The varying aetiological spectrum impacts on the
need for and timing of pericardiectomy.
17
In the Sagrista-Sauleda series, pericardiectomy was not
performed in eight of 15 patients; in five of them owing to a poor
general prognosis (four patients with neoplastic pericarditis)
or a high surgical risk (one patient with radiation pericarditis),
and in three patients (all with idiopathic pericarditis) because
of progressive improvement and eventually resolution of the
illness after pericardiocentesis. Wide anterior pericardiectomy
was performed in seven patients between 13 days and four
months after pericardiocentesis owing to the persistence of
severe right heart failure. The diagnoses in these seven patients
were idiopathic pericarditis in four, radiation pericarditis in one,
tuberculous pericarditis in one, and postsurgical pericarditis in
one.
The patients in our limited series, as in others cases due to
tuberculosis, usually had attendant pericardial calcification with
no room for improvement without pericardectomy. This partly
explains the need for pericardectomy in these patients.
Decision based on timing of presentation and
response to medication
Related to aetiology is the timing of presentation. Transient
sub-acute effusive–constrictive pericarditis is known to resolve
after pericardiocentesis without the need for pericardiectomy.
3,23,24
In fact in two of three patients with idiopathic pericarditis who
had resolution of their symptoms following pericardiocentesis in
the Sagrista-Sauleda series, the onset of their illness was stated
to be very recent. The monitoring of intra-cardiac and intra-
pericardial pressures as part of a pericardiocentesis procedure
has been suggested in patients who present with a sub-acute
course of pericardial tamponade, particularly those in whom the
condition is idiopathic or is related to infection, neoplasm or
rheumatological disease.
2
The duration of pericardial disease in three of our patients
was more than two years, suggesting chronicity and need for
pericardectomy. Although the duration in the fourth and fifth
patients was relatively short, non-resolution of their symptoms
and presence of pericardial calcification in the fourth patient
appeared to be a predictor of need for pericardial stripping.
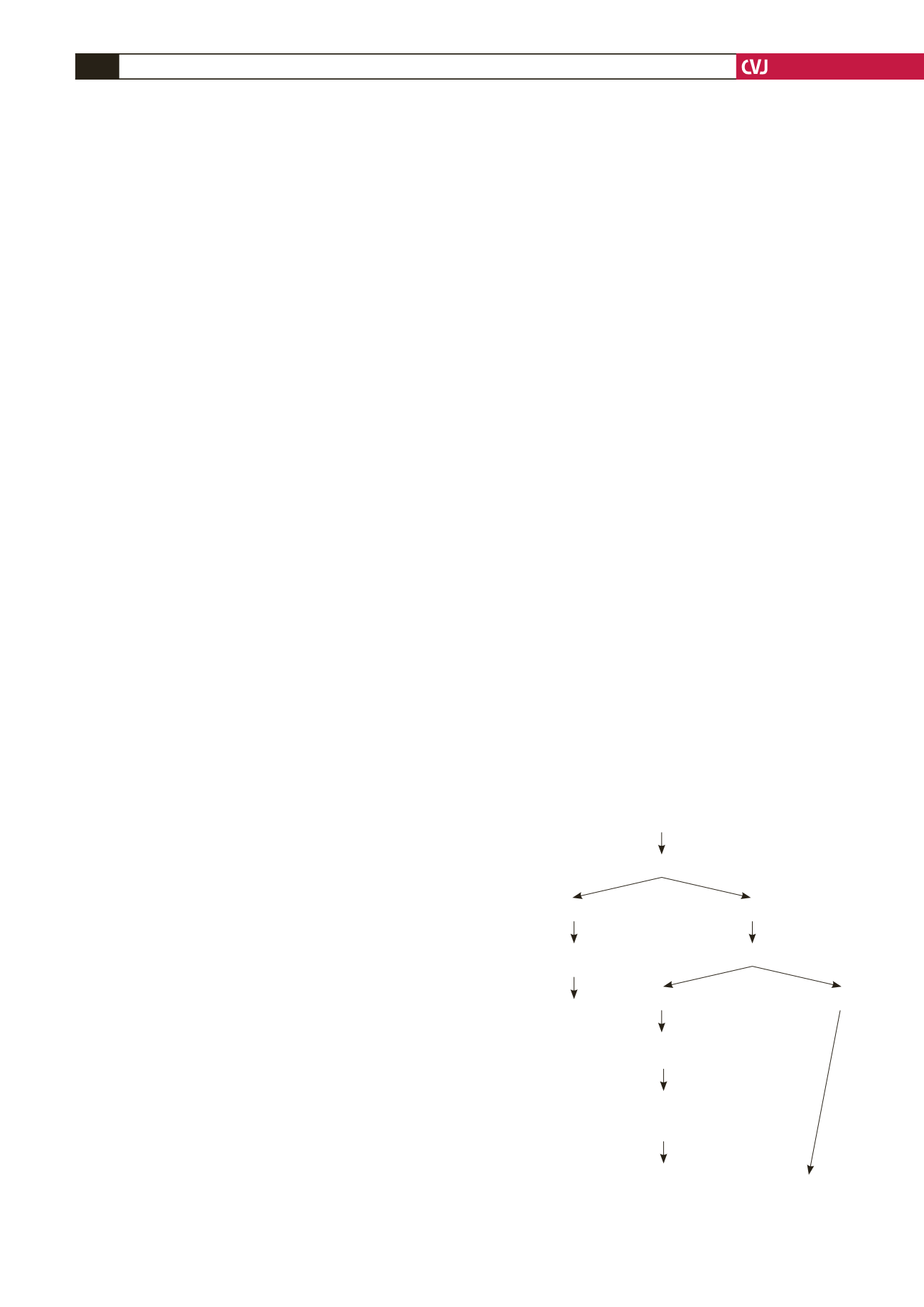
Fig. 5. Potential algorithm for the management of effu-
sive–constrictive pericarditis.
Effusive–constrictive pericarditis diagnosed?
• Based on radiological finding of cardiomegaly
• Evidence of constrictive physiology on echocardiography
Clinical or echo findings of tamponade?
No
Pericardiostomy +
pericardial biopsy
Duration less than 1 year
Yes
No
Medical treatment +/–
pericardiocentesis
Tuberculous/calcification/
persistent symptoms/
elevated venous pressures
Pericardiectomy including visceral pericardium
Yes


