CARDIOVASCULAR JOURNAL OF AFRICA • Vol 23, No 4, May 2012
208
AFRICA
postoperative improvement and was discharged but he
represented three months later with worsening of pre-operative
symptoms. He then had a pericardiectomy, following which he
improved progressively.
Following tube pericardiostomy, DS had very transient
improvement in his symptoms. Repeat lateral chest X-ray showed
evidence of pericardial calcification while echocardiography
showed moderate pericardial effusion and diastolic dysfunction
(Fig. 4). He made a rapid recovery following pericardiectomy.
MNhadminimal improvement following tubepericardiostomy,
remaining dyspnoeic at rest. Postoperative chest radiography
and echocardiography showed pericardial calcification. In
addition, there was a markedly enlarged right atrium, grade
III–IV tricuspid regurgitation and a small right ventricle with
endocardial thickening, suggestive of endomyocardial fibrosis.
We elected to go ahead with a pericardiectomy on account of
the pericardial thickening with calcification. She improved
following pericardiectomy, with NYHA class I status.
OS had pericardiostomy with slight improvement and
was discharged home on anti-tuberculous therapy. He had a
pericardiectomy three months later, during which he had an intra-
operative complication of right ventricular wall injury, which
was promptly repaired. He had an uneventful postoperative
recovery until the 12th and 19th days postoperatively, when
he developed Fournier’s gangrene and upper gastrointestinal
bleeding, respectively. These were successfully managed and he
was discharged home on the 36th day postoperatively.
Discussion
Effusive–constrictive pericarditis is said to be an uncommon
pericardial syndrome.
2
In a prospective study of 1 184 patients
with pericarditis, Sagrista-Sauleda
et al
. reported a prevalence of
only 1.3% among patients with pericardial disease of any type
(15/1 184) and 6.9% among patients with clinical tamponade
(15/218).
3
However, a recent observational study by Mayosi
et al
. reported 28 (15.1%) of 185 patients with tuberculous
pericarditis as belonging to that subset.
4
This is quite similar to
the prevalence of 13% among patients with pericardial disease
of any type in our seven-year review (11/86). We are not aware
of any specific series from Africa.
Patients with effusive–constrictive pericarditis present with
symptoms due to limitation of diastolic filling. These findings
are secondary not only to the pericardial effusion but also
the pericardial constriction. Symptoms and physical findings
vary, while a moderate-to-large pericardial effusion may occur.
Management of effusive–constrictive pericarditis is therefore
fraught with challenges.
The diagnosis is usually made by echocardiography, which
should demonstrate diastolic dysfunction. The diagnosis can
easily be missed by an unwary clinician because of the usual
superimposed features of accompanying pericardial effusion
or tamponade. This may have accounted for the premature
discharge and re-admission of one of our patients (SB).
Pericardial effusion is seen as an echo-free space around
the heart on echocardiography (Fig. 4). The presence of a
large pericardial effusion with frond-like projections and a
thick ‘porridge-like’ exudate is suggestive of an exudate but
not specific for a tuberculous aetiology.
1
Patients with acute
haemorrhagic effusions may have pericardial thrombus appearing
as an echo-dense mass.
5
Small pericardial effusions are only seen posteriorly, while
those large enough to produce cardiac tamponade are usually
circumferential. In large pericardial effusions, the heart may
move freely within the pericardial cavity (‘swinging heart’). In
the parasternal long-axis view, pericardial fluid reflects at the
posterior atrio-ventricular groove, while pleural fluid continues
under the left atrium, posterior to the descending aorta. Rarely,
tumour masses are found within or adjacent to the pericardium
and may masquerade as tamponade.
6
Diagnostic criteria for cardiac tamponade include diastolic
collapse of the right atrial and ventricular anterior free wall, and
left atrial and very rarely left ventricular collapse. Right atrial
collapse is more sensitive for tamponade, but right ventricular
collapse lasting more than one-third of diastole is a more
specific finding for cardiac tamponade. Doppler findings include
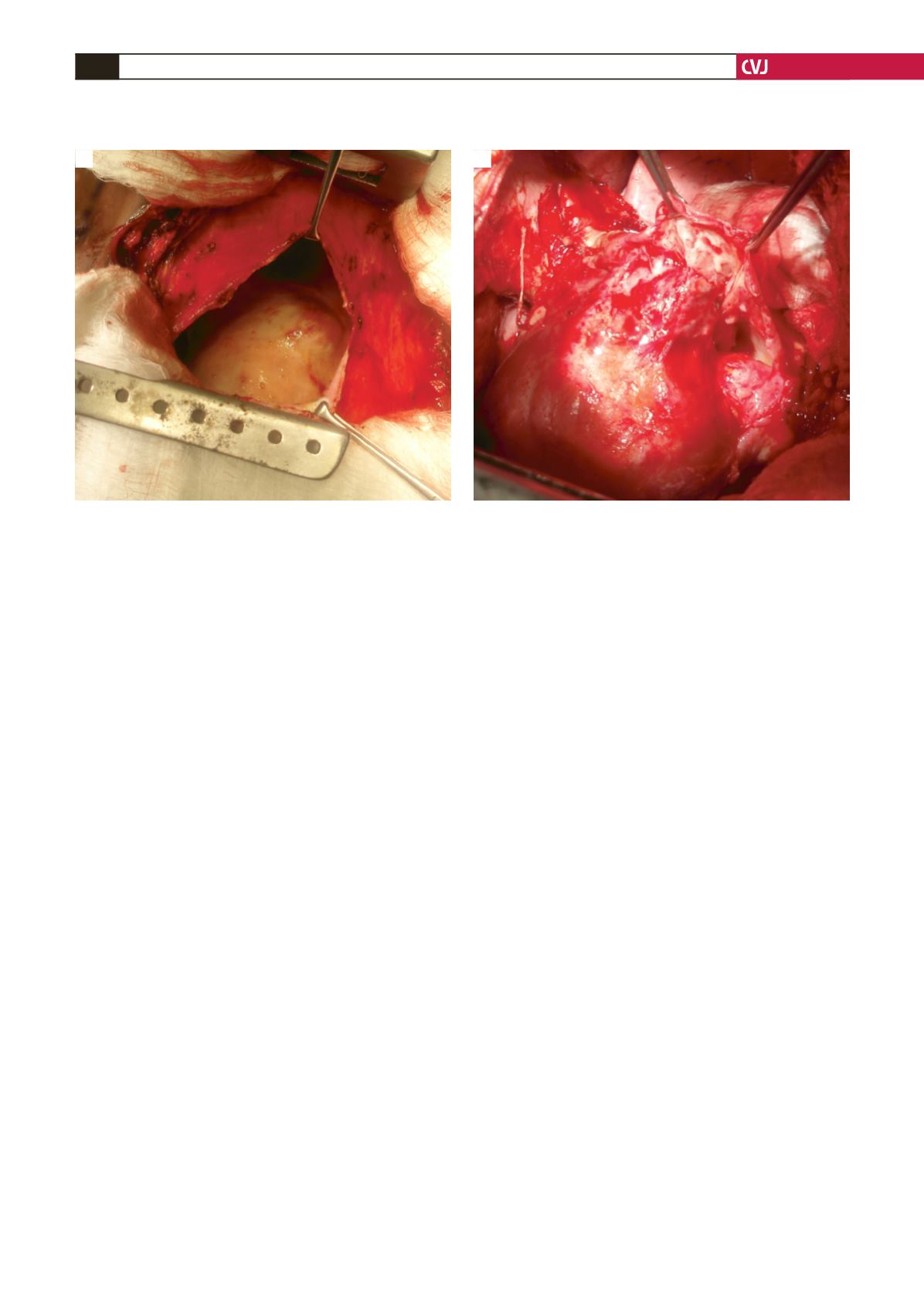
Fig. 3. (A) Thickened pericardium and a large pericardial space. (B) Final phase of visceral pericardial stripping.
A
B


