


















 55 / 68
55 / 68

CARDIOVASCULAR JOURNAL OF AFRICA • Volume 26, No 1, January/February 2015
AFRICA
e5
to be protruding into the aorta due to the shortness of the
LMCA. We therefore realised that the stent had migrated into
the aorta over time and embolised in the femoral artery.
Studies have shown that the incidence of coronary stent
dislodgement towards the peripheral or visceral arterial system
ranges from 0.9 to 8.4%. Stent dislodgement usually occurs with
previously inserted stents during retrieval of the stent–balloon
complex into the catheter.
1,4
Along with this process, impaired
guidance of the catheter or wire, tortuous vessels and severe
calcification may contribute to dislodgement.
1,4
Earlier studies have suggested that migration often occurs
in the early period following coronary stenting. Siani
et al
.
3
reported a case of early coronary stent migration, where the
migrated stent material was detected at the start of the right
common femoral artery.
3
Another case report showed an early
dislodgement of the coronary stent, in which the material
was found in the right posterior tibial artery.
8
In a case report
published by Castiglioni
et al
.,
9
the patient had recurrent angina
pectoris after coronary stenting. The authors detected stent
dislodgement into the ascending aorta.
9
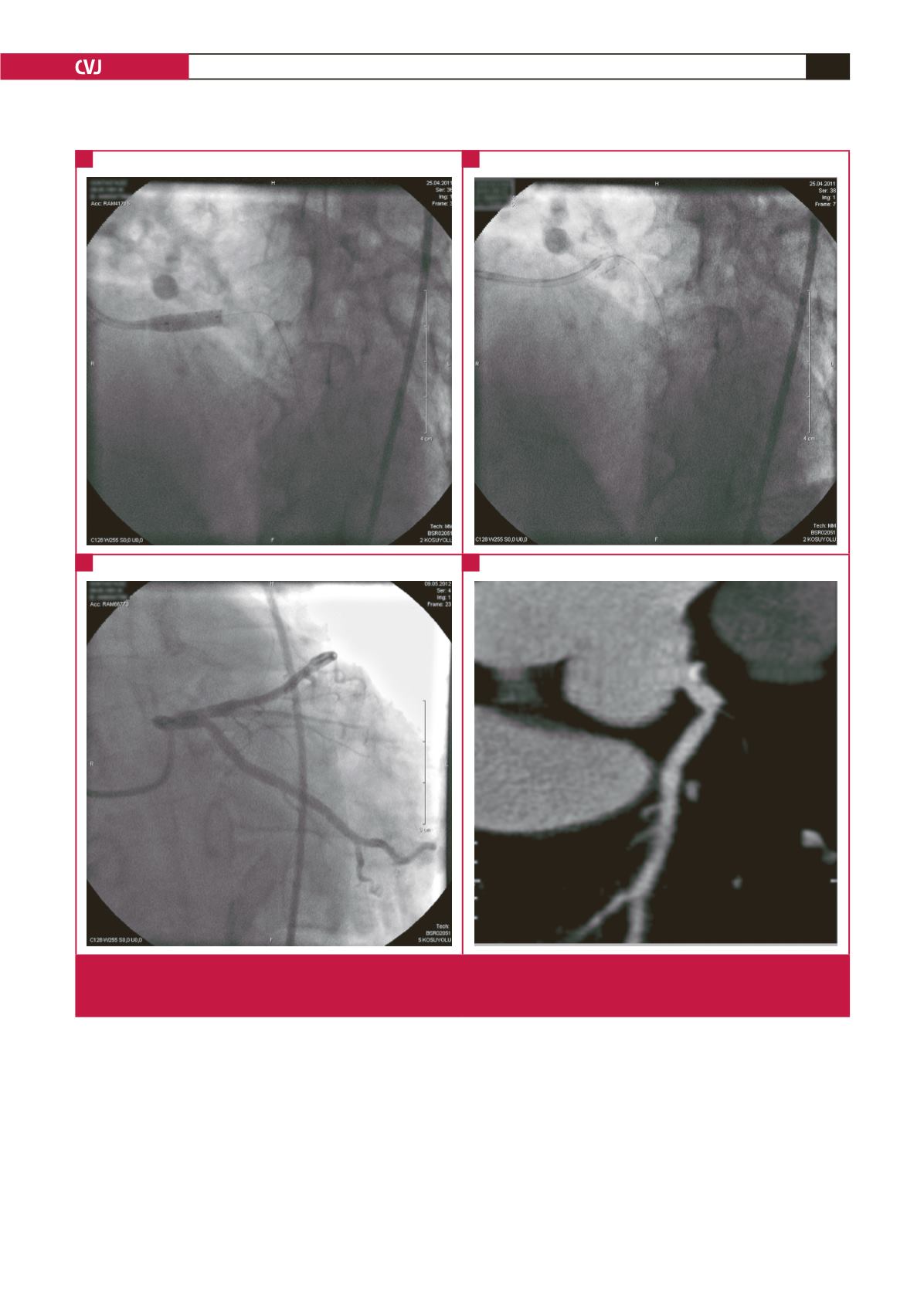
Fig. 1.
A, B: Coronary angiography showing the stent implanted in the LMCA during baseline coronary angiography. C: Coronary
angiography showing absence of the stent in repeated coronary angiographs. D: Computed tomography coronary angiogra-
phy showing the absence of the LMCA stent.
A
C
B
D