
















 58 / 68
58 / 68

CARDIOVASCULAR JOURNAL OF AFRICA • Volume 26, No 3, May/June 2015
e8
AFRICA
A pericardial biopsy showed a cellular tumour comprising
vasoformative spindle cells with extravasation of red blood cells
and eosinophilic bodies. Moderate nuclear pleomorphism and
a brisk mitotic count were seen. This was consistent with an
angiosarcoma (Fig. 2).
The patient was referred to oncology care after debulking and
he received a pulse of chemotherapy (vincristine, doxorubicin
and cyclophosphamide). He became paraplegic and eventually
died five months after his initial presentation.
Discussion
Primary cardiac tumours are rare and angiosarcoma is the most
frequent primary malignant cardiac tumour.
6
Angiosarcomas
of the pericardium are rare but there have been several case
reports.
7-10
They usually occur in the third to the fifth decade of
life and are more common in males. By the time these tumours
are diagnosed, 66 to 89% have metastases. They have a poor
prognosis. The mean survival is six to 11 months. Metastatic
disease is frequent at the time of presentation, mainly to the
mediastinal lymph nodes, lung and vertebrae. Our patient’s
tumour was quite invasive and had metastases to several
vertebrae.
In this patient, the initial radiological investigation was
an echocardiogram, which revealed a fibrinous pericardial
effusion. Echocardiography is usually the initial diagnostic
tool for cardiac tumours. Transthoracic and transoesophageal
echocardiography have a sensitivity of 93 and 97%, respectively,
for detecting cardiac masses.
11
These however are operator and
technique dependant.
CT and magnetic resonance imaging reveal more detail in
terms of cardiac soft tissue as well as extracardiac extension
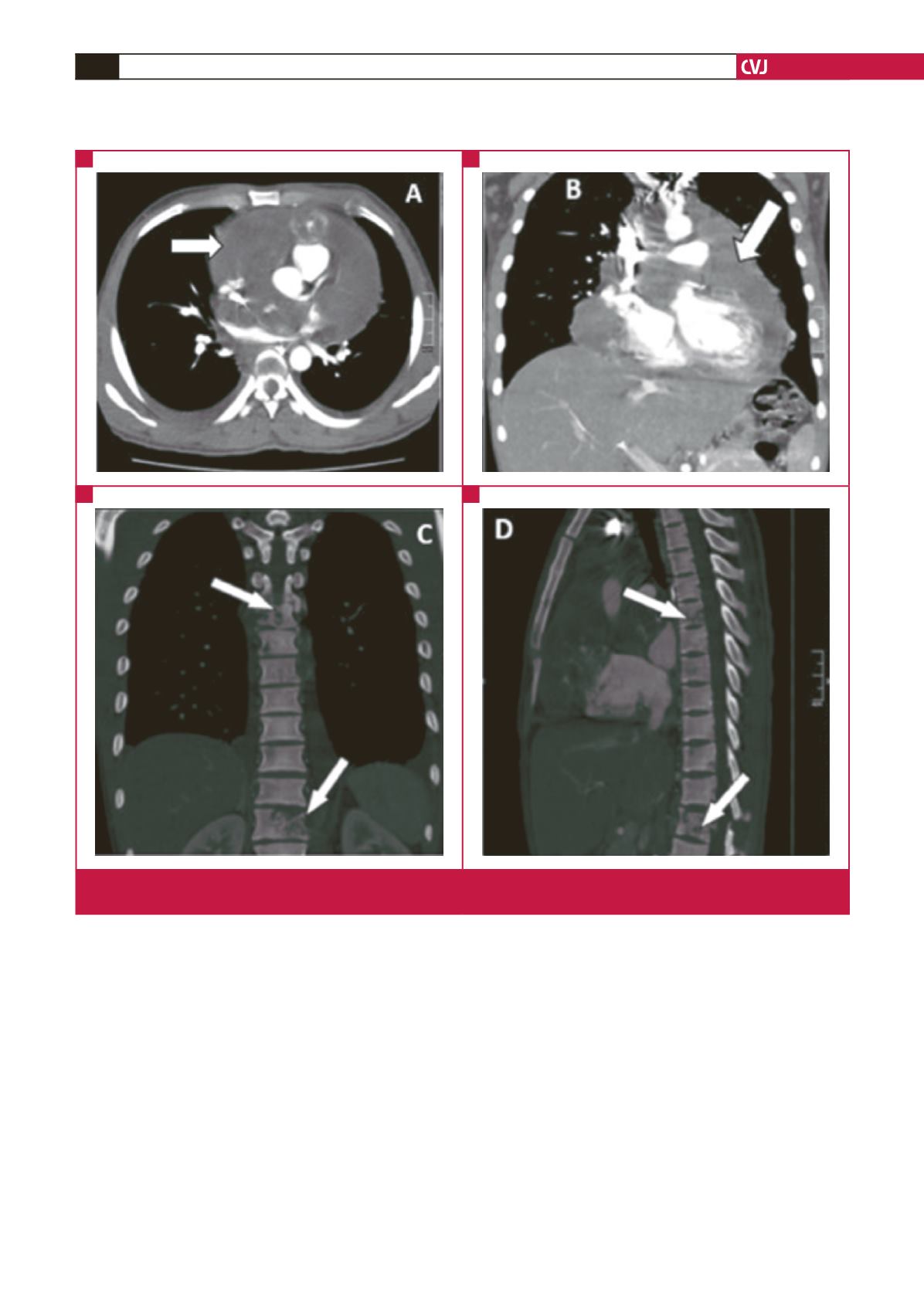
Fig. 1.
CT images of pericardial tumour and vertebral invasion. (A, B) Tumour surrounding all cardiac chambers. (C, D) Thoracic
and lumbar vertebral invasion by tumour.
A
C
B
D