
















 22 / 76
22 / 76

CARDIOVASCULAR JOURNAL OF AFRICA • Volume 28, No 1, January/February 2017
20
AFRICA
Statistical analysis
SPSS 21.0 software (SPSS Inc, Chicago, IL, USA) was used for
the statistics. For data processing, besides descriptive statistical
methods such as frequency, percentage, mean values and
standard deviation, the Kolmogorov–Smirnov test was used to
evaluate the data distribution. For comparison of the parameters
in specific groups, the Wilcoxon
Z
-test and kappa analysis were
used. Survival analysis was obtained with the Kaplan–Meier
method. The results were evaluated for significance (
p
<
0 .05).
Results
Between November 2010 and April 2012, 30 patients (75% male)
with a mean age of 68
±
5.04 years underwent epicardial LV
lead placement following a failed attempt at percutaneous CRT.
Table 1 summarises the baseline demographics for the patients
included in this study.
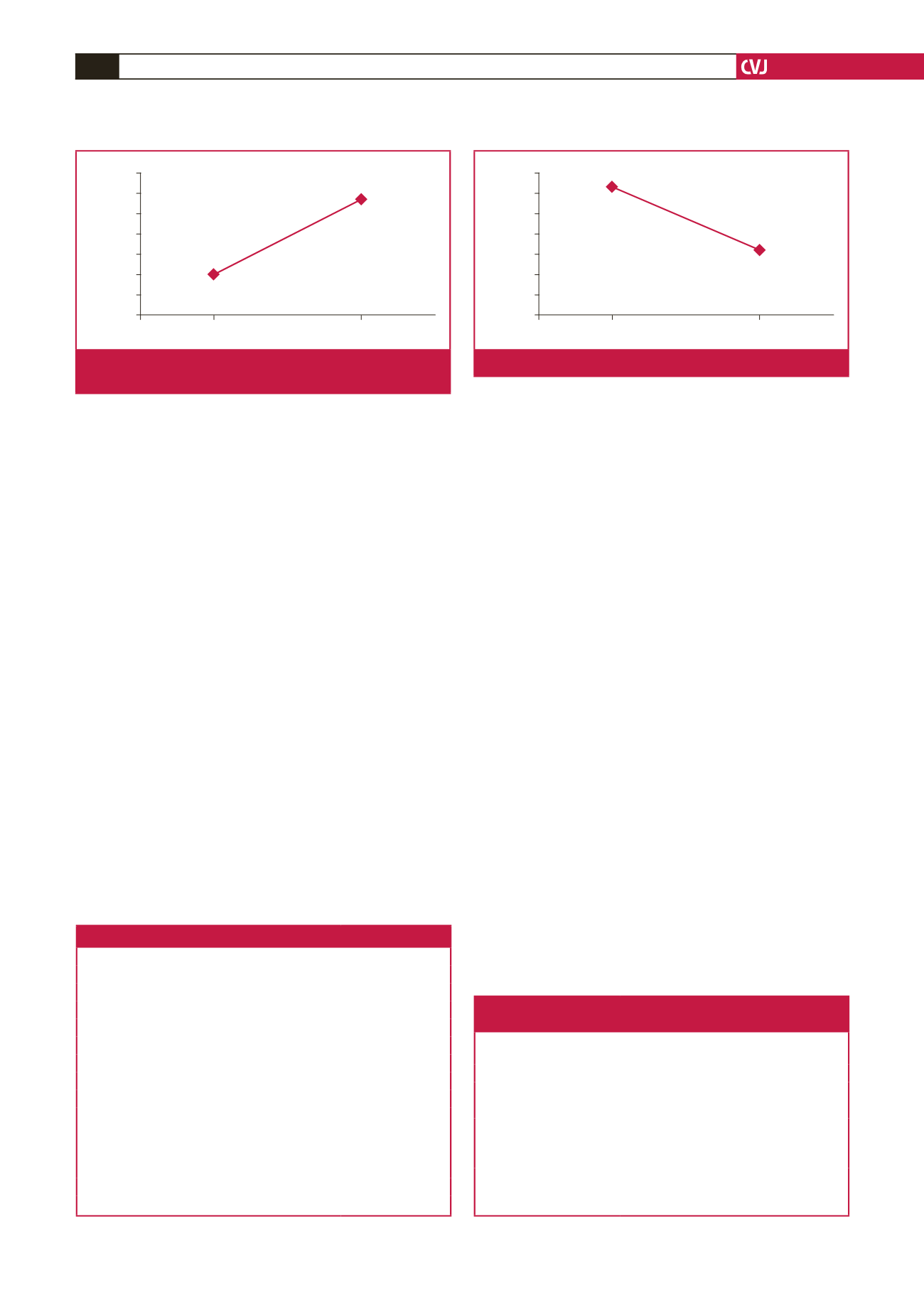
All patients were in NYHA functional class III or IV.
Pre-procedure mean LVEF was 28.1
±
4.5% and ejection fraction
improved to 31.7
±
5.1% post procedure (Fig. 1).
The pre-surgery QRS duration reduced from 171.7
±
10.8
to 156.2
±
4.4 ms post surgery (Fig. 2). In addition there was a
significant reduction in LVEDD, from 6.98
±
0.8 to 6.72
±
0.8
mm (
p
<
0 .05), but no change in left ventricular end-systolic
dimension (LVESD) and in severity of MR (
p
>
0 .05) (Table 2).
Patients spent an average of 1.3
±
0.4 days in the intensive
care unit post operation. Mean length of hospital stay was 4.9
±
2.2 days. Mean duration (skin-to-skin) of procedure was 52.6
±
12.5 minutes for left ventricular lead implantation through the
mini-thoracotomy.
All patients had successful surgical LV lead placement. There
was no procedure-related mortality. Intravenous therapy was
commonly administered, with diuretics used in 92% of patients
and inotropes in 10% of patients.
In total, one patient underwent heart transplantation within
five months of surgical lead placement. Ten patients (30%) died
during the observation period. The mean follow-up time was
40.4 months (Fig. 3).
Discussion
CRT has been well-documented to improve left ventricular
ejection fraction, heart failure symptoms and survival.
2
A
percutaneous transvenous approach for CRT depends on several
factors, such as coronary sinus anatomy, and it can be time
consuming.
4
If there are small coronary veins, it may not be
feasible, whereas in the case of large coronary veins, it is often
associated with changes in pacing threshold. Furthermore, life-
threatening complications such as coronary sinus perforation
may occur.
5
Sub-optimal LV lead positioning may lead to
unfavourable clinical outcomes following CRT.
The advantage of surgical epicardial LV lead positioning is
that direct visualisation helps to select the most suitable surface
and avoid epicardial fat or fibrosed areas, which can cause
changes in pacing thresholds. Mair
et al
.
6
recommend that CS
lead implantation should be stopped if the procedure exceeds
two hours. In our cases, it took 52.6
±
12.5 minutes from skin
incision to completion of LV lead implantation.
Table 1. Baseline clinical demographics of patients
Variables
Number (%)
Gender
68
±
5.04
Male
2 (75)
Female
8 (25)
Aetiology
Non-ischaemic cardiomyopathy
8 (25)
Ischaemic cardiomyopathy
22 (75)
Co-morbidities
Diabetes mellitus
13 (43)
Hypertension
18 (60)
Previous myocardial infarction
17 (56)
Chronic obstructive pulmonary disease
8 (26)
Chronic renal failure
9 (30)
Previous cardiac surgery
7 (23)
Previous pacemaker/ICD
10 (33)
Table 2. Clinical and echocardiographic outcomes
following surgical lead placement
Parameters
Pre-procedural
outcome
Post-procedural
outcome
p
-value
LVEDD (mm)
6.98
±
0.8
6.72
±
0.8 0.030
LVESD (mm)
5.97
±
0.8
5.90
±
0.8 0.128
EF (%)
28.1
±
4.5
31.7
±
5.1 0.000
Moderate or severe MR,
n
(%)
6 (42)
7 (43)
0.080
QRS (ms)
171.7
±
10.8 156.2
±
4.4 0.000
LVEDD, left ventricular end-diastolic dimension; LVESD, left
ventricular end-systolic dimension; EF, ejection fraction; MR, mitral
regurgitation.
Pre-procedure
Post-procedure
33
32
31
30
29
28
27
26
EF (%)
Fig. 1.
Pre- and post-procedural mean left ventricular ejection
fraction.
Pre-procedure
Post-procedure
175
170
165
160
155
150
145
140
QRS (ms)
Fig. 2.
Pre- and post-procedural mean QRS duration.