
















 80 / 84
80 / 84

CARDIOVASCULAR JOURNAL OF AFRICA • Volume 29, No 2, March/April 2018
e10
AFRICA
our tertiary hospital, which was at least 24 hours later, revealed
sinus rhythm with evidence of a recent extensive antero-septal
myocardial infarction (Fig. 3). Her chest X-ray is shown in Fig. 4.
Echocardiography revealed preserved LV function with an
ejection fraction of 62% and regional wall motion abnormalities,
including antero-septal and infero-basal hypokinesia. Coronary
angiography revealed a sub-totally occluded LAD (Fig. 5).
Percutaneous revascularisation was performed where a bare-
metal stent was successfully deployed with no peri-procedural
complications (Fig. 5). Strict radiation protective measures of
the foetus were undertaken during the procedure.
An elective caesarean section was performed two weeks later,
when a 2.2-kg female baby was delivered with no peri-operative
complications. During her cardiology follow up, she reported
severe prolonged rest pain, which was attributed to poor
compliance. Her management was optimised and her symptoms
improved.
Discussion
Acute myocardial infarction
In the largest series of AMI in pregnancy where 125 patients
were reported, the authors discovered the highest incidence of
AMI in the third trimester, and most importantly, in multigravid
women older than 33 years of age.
1,2,10-12
In the same report, a
coronary angiography was performed in 54% of the patients;
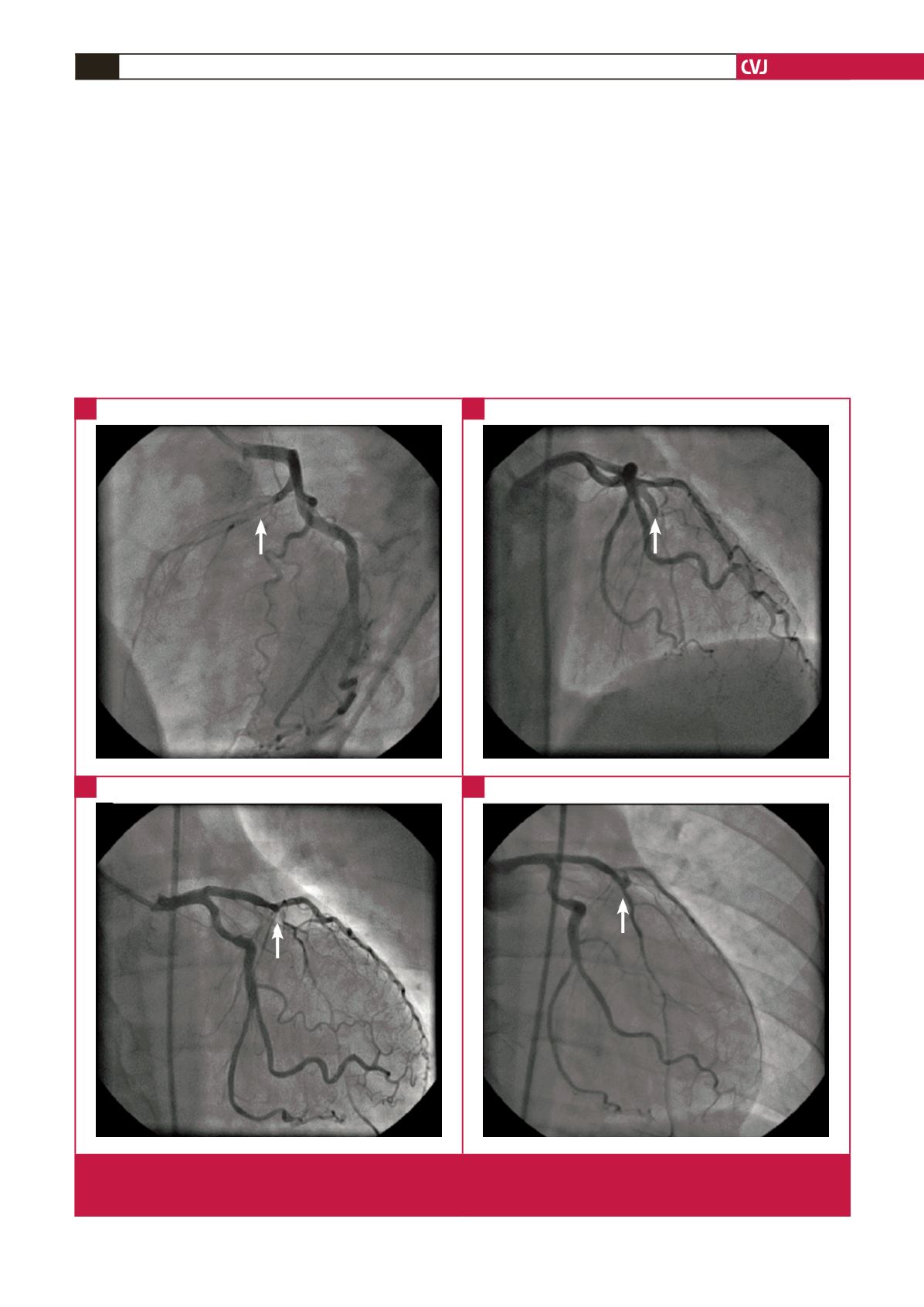
Fig. 5.
Patient 3. (A–C) Coronary angiogram showing the sub-totally occluded left anterior descending coronary artery (LAD, indi-
cated by the white arrows). (D) Improved flow post-PCI and stenting to the proximal LAD with TIMI 3 flow to the distal vessel
(white arrow).
A
C
B
D