


















 19 / 62
19 / 62

CARDIOVASCULAR JOURNAL OF AFRICA • Volume 31, No 1, January/February 2020
AFRICA
17
too much compression of the heart and further haemodynamic
disturbances, but we still had enough tension to retract the heart
and support the stabilisation system. Anastomoses were thus
done with direct access and without excess manipulation of the
heart (Fig. 1).
During right coronary artery (RCA) anastomosis, the
operating table was positioned away from the surgeon and the
anastomosis was perfomed with gauzes and the suction system
was used to create a more stable state (Fig. 2). When doing
bypasses to the circumflex branches [obtuse marginal (OM) or
posterolateral (PL) arteries], the operating table was positioned
at 20 degrees Trendelenburg and turned to the right side. No
apical holder was used in any patient. During anastomosis on the
posterolateral surface, the heart was retracted more firmly to the
right side with gauzes and the suction system (Fig. 3).
All distal anastomoses were performed using intracoronary
shunt, except for total occlusion. After completion of the
anastomoses, 50–100 IU/kg protamine (half dose) was
administered and the operation was terminated.
The patients were ventilated with high frequency and low tidal
volume (350–400 ml) to prevent movement during anastomosis.
Tidal volume was increased when there was a problem with
saturation in the arterial blood gas values. No patient had an
oxygenation problem during the operation.
The patients were monitored and followed closely in the
intensive care unit. Low-molecular-weight heparin was given to
all patients for four to six hours postoperatively.
In this study, haemodynamic instability, ventricular fibrillation
and anastomotic difficulty were the main criteria for conversion
to on-pump surgery.
Statistical analysis
SPSS statistics for Windows version 22.0 (SPSS Inc Chicago, IL,
USA; released 2008) was used for statistical analysis. The paired-
samples
t-
test was used to compare repeated measurements. Since
there was only one group of patients, descriptive studies were
chosen;
p-
values
<
0.05 were considered to indicate statistical
significance.
Results
The study included 606 OPCAB cases performed in a single
centre between January 2014 and December 2018, and 21.8%
(132) of our patients were female and 78.2% (474) were male.
The mean age was 62.25
±
9.47 (min–max 32–86 years) years.
Table 1 shows the baseline characteristics of our patients.
When cardiac function was examined, it was seen that 10.1%
(
n
= 61) of our patients had low left ventricular ejection
fraction (LVEF). In these patients, excessive volume overload
was avoided in the peri- and postoperative period. Postoperative
findings are given in Table 2.
In routine practice in our clinic, when starting inotropic
support, dopamine and noradrenaline infusion are the first
choice. More than two inotropic supports were not used in our
study. The mortality rate was 1.7% (
n
= 10) in 606 cases and only
two patients suffered a cerebrovascular incident (CVI). These
patients recovered without neurological sequelae. Two patients
(0.3%) were converted to on-pump surgery because of ECG
changes (ST elevation) and were haemodynamically affected
despite interventions. No additional morbidity and mortality
was observed in these patients.
The number of distal anastomoses in our study is shown in
Table 3. In Table 4, our six-month postoperative LVEF results
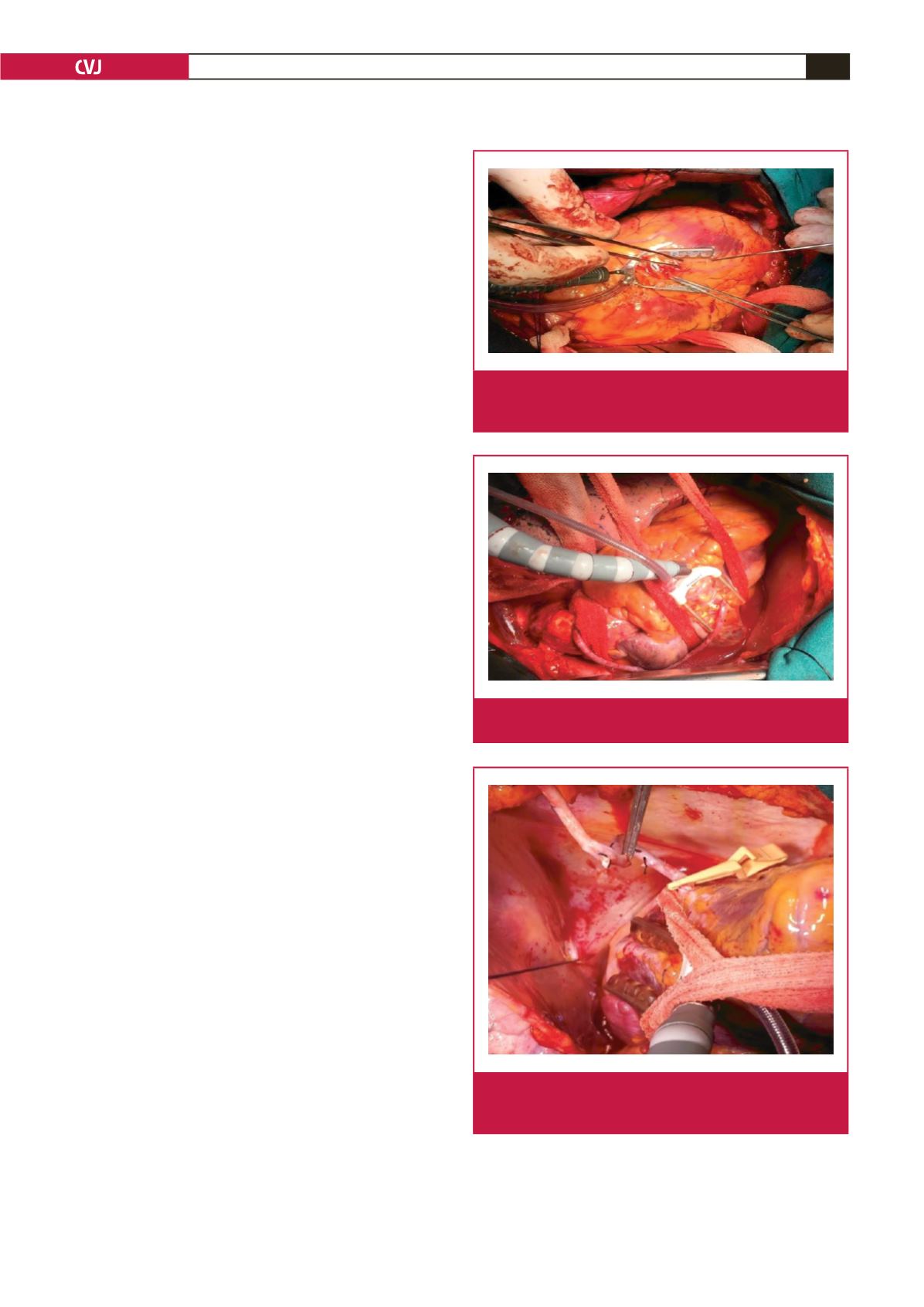
Fig. 1.
Anastomosis on the anterior face of the heart with the
help of a deep pericardial suture and the Octopus
®
system.
Fig. 2.
Anastomosis on the inferior face of the heart with the
help of the Octopus
®
system and moistened gauzes.
Fig. 3.
Sequential anastomoses on the posterolateral face of
the heart with the help of the Octopus
®
system and
moistened gauzes.