


















 58 / 64
58 / 64

CARDIOVASCULAR JOURNAL OF AFRICA • Volume 31, No 5, September/October 2020
278
AFRICA
was normal with an EF of 75%, while the diastolic function was
worsened with E (1.0 m/s)/A (0.6 m/s) = 1.7, e
′
(3.5 m/s)/a
′
(2.8
m/s) = 1.2 and E/e
′
= 28.5. A 3.7-mm pericardial effusion was
also identified on the roof of the right atrium.
In addition to diuretics and aldosterone receptor antagonists,
as well as beta-blockers to control the fast heart rate, the patient
received a five-day intravenous dexamethasone infusion at a
dosage of 10 mg once per day, and oral prednisone and warfarin
at the dosage of 75 and 3.5 mg once per day, respectively.
Additionally, cytotoxic hydroxycarbamide, a cytotoxic agent,
was added at a dosage of 500 mg twice per day.
The patient’s symptoms of cough and dyspnoea were
markedly alleviated one week later. His temperature returned
to normal, the rash completely disappeared, and the moist
rales disappeared on both lungs. Repeat chest X-ray revealed
substantially reduced infiltrating shadows with no evidence of
pleural effusion. The WBC count was decreased to 18.54 × 10
9
cells/l, with 37.7% eosinophils and a total blood count of 6.99 ×
10
9
cells/l. The patient was discharged and closely followed up by
his field physicians.
Discussion
IHES is a rare eosinophilic proliferative disease involving
multiple vital organs. It more often occurs in men, and the
ratio of male-to-female is about 9:1.
4
Studies have reported that
cardiac involvement occurs in more than 50% of IHES patients
and is the leading cause of death. The in-hospital death rate due
to cardiac involvement secondary to IHES was reported in one
study to be 12.5%.
7
Eosinophil-mediated cardiac injury occurs in three stages:
5,6
(1) an early necrotic stage characterised by the formation
of myocardial necrosis and micro-abscess due to eosinophil
infiltration and toxic cationic protein released from degranulation
of the eosinophils; (2) an intermediate thrombotic stage
manifesting as the formation of thrombi on the surface of
damaged myocardium; and (3) a late fibrotic phase characterised
by the formation of endomyocardial fibrosis and scar, which is
frequently associated with cardiac diastolic dysfunction and even
restrictive cardiomyopathy. Progressive extensive endomyocardial
fibrosis may also attack the chordae tendineae and papillary
muscles, leading to valvular insufficiency.
10
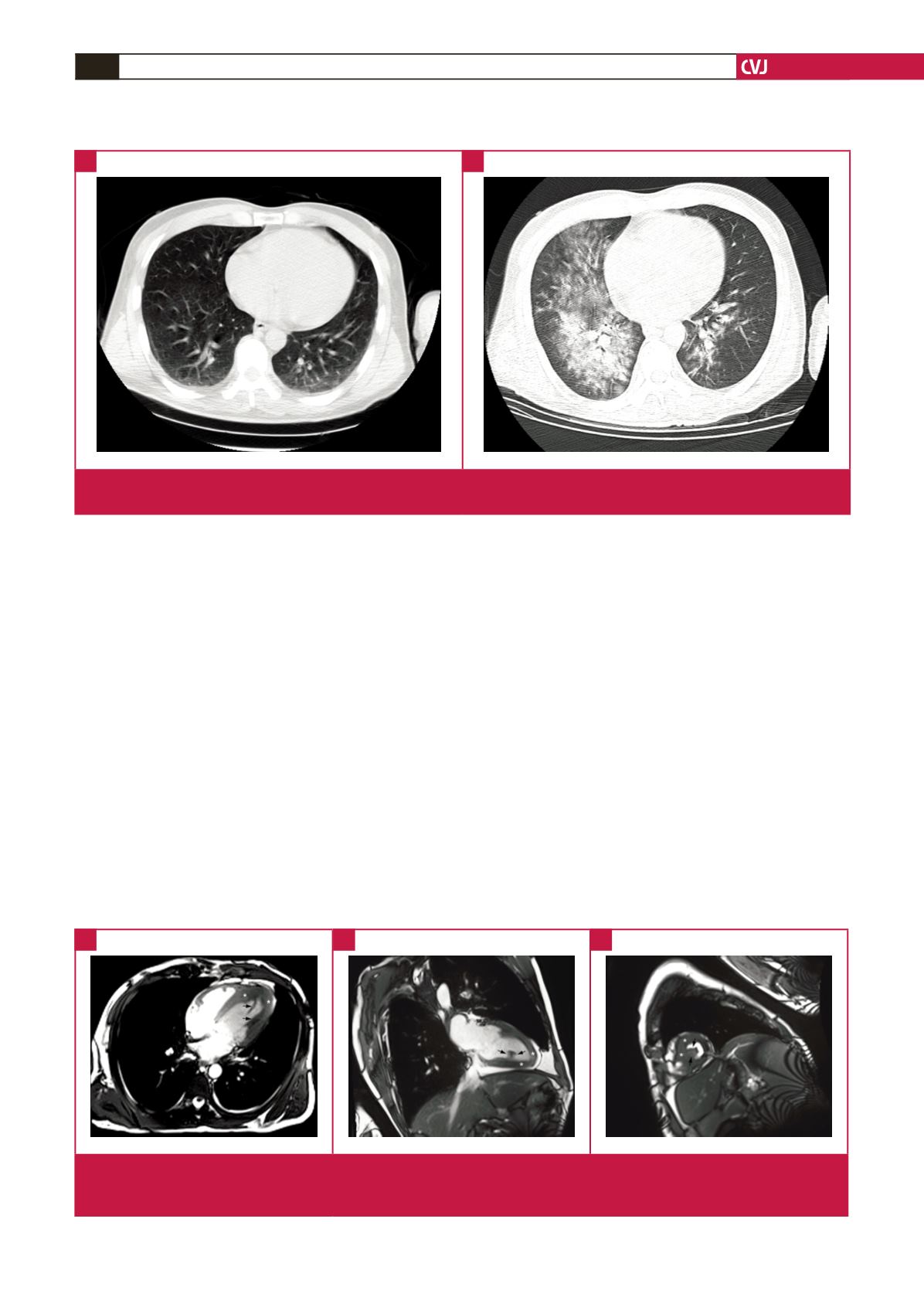
Fig. 4.
Chest CT. A: image on the first admission showing slightly increased bilateral bronchovascular shadows on the lungs. B:
image on the second admission showing large, flaky, high-density infiltrates throughout the right and inferior left lung.
A
B
Fig. 5.
Frozen images of cine-cardiac magnetic resonance true fast imaging with steady-state free precession sequences. A: four-
chamber view. B: two-chamber view. C: short-axis view. The white asterisks indicate the markedly thickened endocardium
and black arrows indicate the thrombi within the LV cavity.
A
B
C