


















 59 / 64
59 / 64

CARDIOVASCULAR JOURNAL OF AFRICA • Volume 31, No 5, September/October 2020
AFRICA
279
Mimicking acute coronary syndrome (ACS), IHES-mediated
myocardial necrosis may manifest as chest pain, abnormal
ischaemic ECG changes and elevated troponin-I,
7
which may be
neglected by clinical doctors. Our presenting patient was initially
misdiagnosed as ACS by the emergency room doctor; however,
the negative coronary angiogram excluded coronary artery
anomalies. Additionally, it should be noted that normal CK
and CK-MB levels with only increased troponin-I and without
enzymatic dynamics are not likely to confirm a diagnosis of
ACS. Due to the highly elevated peripheral eosinophil numbers
and atypical near-mature eosinophils in the bone marrow, as well
as finally excluding secondary causes of hypereosinophilia, the
patient was diagnosed with IHES and IHES-mediated cardiac
injury.
TTE is the most common and convenient modality to identify
cardiac injury in clinical practice. Typical findings of IHES-
mediated cardiac involvement on TTE include endomyocardial
thickening, mural thrombus, valvular insufficiency and
restrictive diastolic dysfunction.
11,12
In this report, the findings of
thickened endomyocardium, ventricular diastolic dysfunction,
enlarged bilateral atria, elevated pulmonary arterial pressure and
aggravated valvular regurgitations on TTE were consistent with
a diagnosis of IHES-mediated cardiac damage.
The thickened endomyocardium may be explained by the
extensive formation of endomyocardial fibrosis and scar, and
the multiple valve regurgitations can be ascribed to the adverse
involvement of chordae tendineae and/or papillary muscles
secondary to IHES. Impaired LV diastolic function may suggest
restrictive cardiomyopathy resulting from substantially thickened
ventricular endomyocardium and reduced compliance in the LV
myocardium. Additionally, the IHES-mediated restrictive LV
filling dysfunction limits blood evacuation from the atria into
the ventricles, thereby, leading to volumetric dilation of both
atria and subsequent elevated pulmonary artery pressure. These
abnormalities on TTE strongly indicated that the patient’s IHES-
mediated cardiac injury had progressed into the final stage.
CMR has been validated as a fairly accurate method of
detecting cardiac injury in the clinic.
13,14
In the present case,
the LV intra-cavity blood, thickened LV endomyocardium
and attached LV mural thrombus showed different intensities
of signal on the frozen cine-CMR images, thereby facilitating
identification of LV thrombotic lesions from the attached
thickened LV endomyocardium.
13,14
Pulmonary infiltration has seldom been reported in IHES
patients.
8
In the present case, no obvious abnormality was
found on chest CT during the first admission, whereas large,
flaky, high-density infiltrating lesions had developed rapidly
within one month after hospital discharge. The fact that the
infiltration shadows were markedly resolved after treatment
with glucocorticoid and hydroxycarbamide without antibiotics
suggests that the pulmonary lesions were related to IHES.
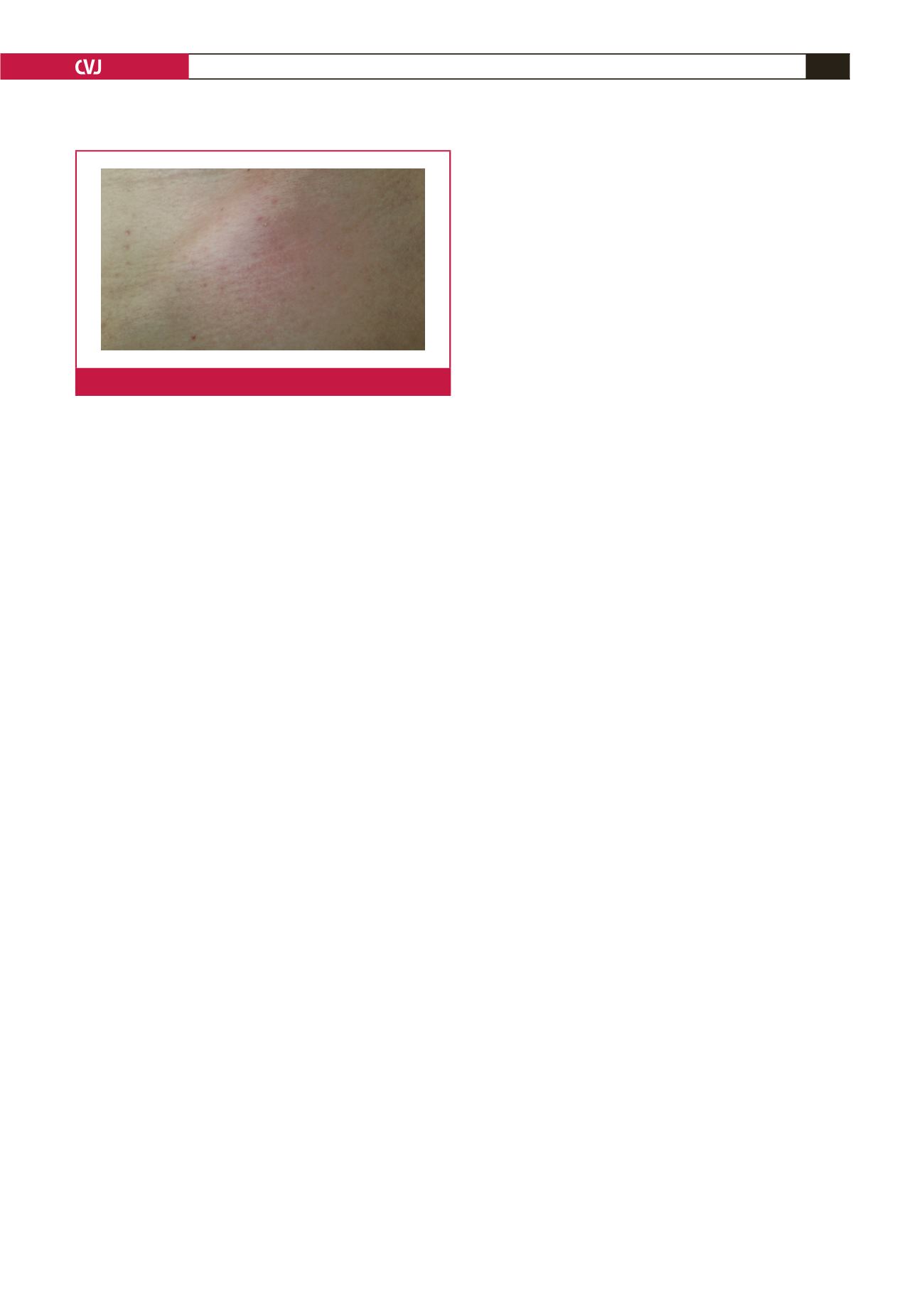
Skin damage resulting from a toxic mediator released from
the degranulation of eosinophils has been reported in 12 to
15% of IHES patients.
9
Typical symptoms of skin involvement
secondary to IHES may include angioneurotic oedema, urticaria
or pruritic papules.
9
In the present case, a rash was apparent
throughout the patient’s trunk and limbs on the second hospital
admission. The rapid disappearance of the rash with combined
therapy of glucocorticoid and hydroxycarbamide suggests that
the skin lesion was IHES related.
In a review of the literature, the objective of IHES
treatment is to reduce the number of eosinophils, as well as
to minimise organ injury and thromboembolic complications.
Glucocorticoids are the first-line drug for IHES patients. If
glucocorticoids are ineffective or a minimum maintenance dose
of > 10 mg/d is required,
α
-interferon or cytotoxic agents, such
as hydroxyurea, vincristine, etoposide, chlorambucil, cladribine
and cyclosporine may be added. Targeted therapeutic drugs,
including imatinib mesylate, anti-IL-5 (mepolizumab) and anti-
CD52 (alemtuzumab) monoclonal antibody, as well as allogeneic
haematopoietic stem cell transplantation may be options for
refractory IHES patients.
15,16
In this report, glucocorticoids were initially effective for
the patient; however, treatment with glucocorticoids was
interrupted after hospital discharge for the patient’s own reasons,
leading to a rapid deterioration in his condition. After the
glucocorticoids were resumed and hydroxyurea was added, the
patient’s condition improved. The markedly decreased peripheral
eosinophils and the reduced infiltrating lesions of the lungs and
skin demonstrated that the combined therapy of glucocorticoids
and hydroxyurea was effective for this IHES patient.
IHESpatients generally showa trend towardhypercoagulation.
It is unclear whether prophylactic anticoagulants should be given
to IHES patients; however, if there is any evidence of cardiac
thrombosis, aggressive anticoagulation therapy is warranted.
15
In our case, the LV thrombus was diagnosed by CMR, therefore
timely and adequate heparin and warfarin anticoagulants were
administered.
In a review of literature, surgical thrombectomy, endocardium
resection and valvular replacement are appropriate options for
some refractory IHES patients. Heart transplantation may be the
last resort for those patients with end-stage cardiac damage.
17,18
Conclusion
IHES is an eosinophilic proliferative disorder involving multiple
vital organs. IHES-mediated cardiac injury mimics ACS, which
may be under-recognised by clinicians. Combined therapy with
glucocorticoids, hydroxyurea and wafarin was effective for our
IHES patient.
This case presentation is supported by the Jilin Province Science and
Technology Development Programme, the Natural Science Foundation (no.
20200201332IC) and the Science and Technology Bureau of Jilin Province,
China (grant no. 20190303182SF).
Fig. 6.
Rash on the skin of the trunk.