
















 40 / 84
40 / 84

CARDIOVASCULAR JOURNAL OF AFRICA • Volume 29, No 2, March/April 2018
102
AFRICA
same day as patient visits (1/7), between one and seven days after
visits (5/7) or over seven days after visits (1/7).
The majority of sites had access to adequate resources for
conducting electrocardiograms (ECGs) and echocardiograms
(echos). Baseline echos were conducted on-site at 27/30
respondents’ sites and baseline ECGs were conducted on-site at
26/30 sites. While 26/30 respondents always or usually had access
to ECGmachines, 2/30 sometimes or seldom had access. Twenty-
five/30 respondents always or usually had access to ECG paper
while 2/30 sometimes or seldom had access.
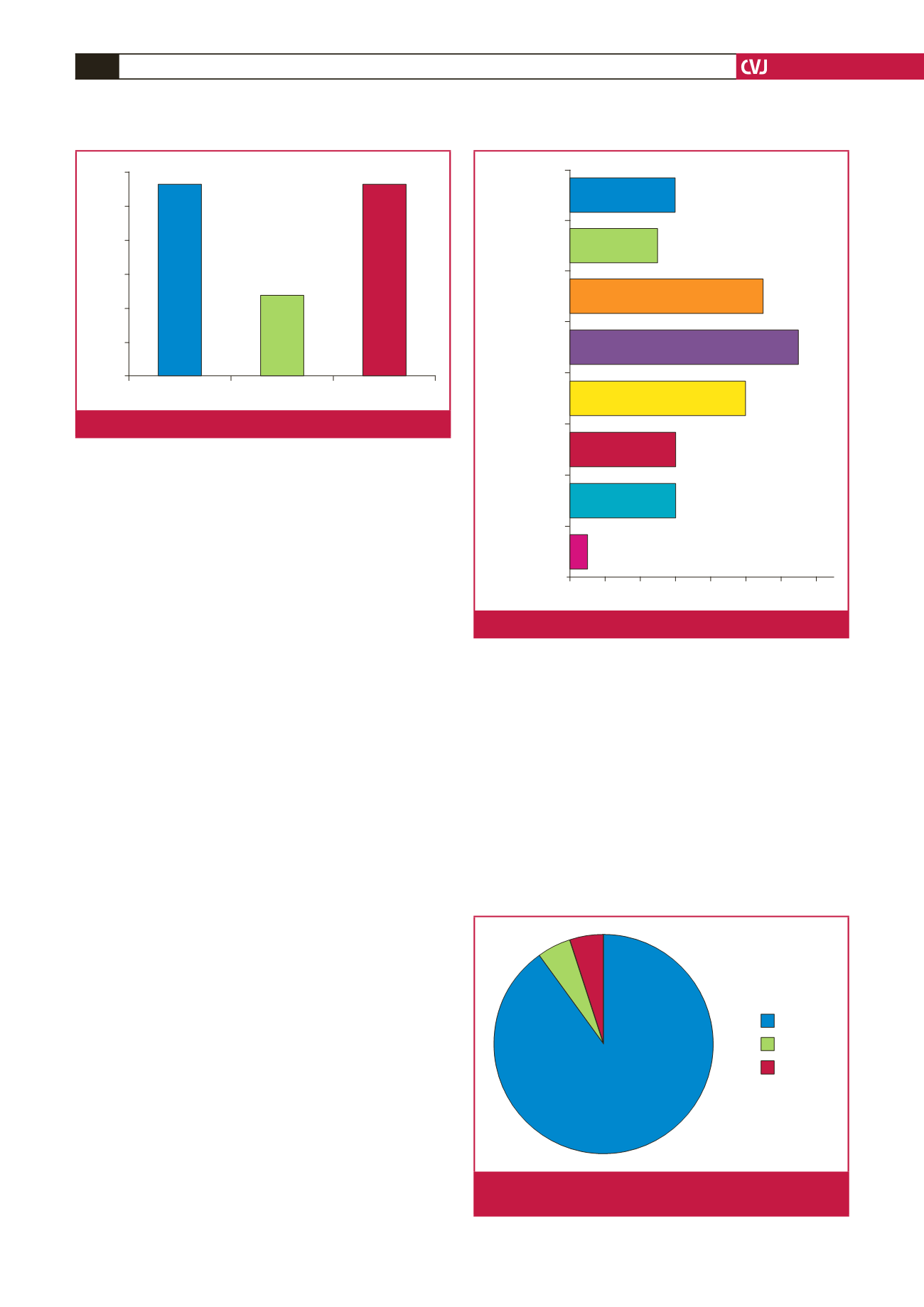
The majority of respondents experienced drug stock-out
problems for their RHD patients, including penicillin (19/30),
anticoagulants (17/30) and other cardiac drugs such as digoxin,
ACE inhibitors, spironolactone and captopril (19/30) (Fig. 6).
On-site internet access varied across sites. For example,
REMEDY e-mail was either provided by respondents’ work
facilities (15/30) or by personal devices and funds (13/30)
throughout the study.
Several sites purchased supplies for conducting the REMEDY
study. Items bought included telephones (6/30), computers (6/30),
airtime (10/30), scanners, copiers and fax machines (13/30),
patient binders, files and stationery (11/30), echo machines
(5/30), ECG machines (6/30) and other supplies not mentioned
in the survey (1/30) such as furniture. Seven/30 respondents did
not purchase anything for conducting REMEDY (Fig. 7).
Telephone interview
Clinical management: almost all responses (17/19) were positive
when asked whether participation in REMEDY changed their
management of RHD patients (Fig. 8). Changes included more
rigorous use of penicillin prophylaxis and anticoagulation,
increased efforts to reduce loss to follow up, establishment of
independent RHD clinics, more regular INR management,
higher-quality standards for echocardiography, improved
knowledge concerning early symptoms of RHD, and increased
efforts to provide family planning counselling to post-menarchal
females. For example, one participant remarked, ‘Before
REMEDY, we were not very keen on important interventions
like family planning and mandatory injections. REMEDY led us
to be more vigilant, to encourage family planning and to make
sure our RHD patients are getting regular medications. It has
improved the care for these patients’.
Research participation: for 15/19 respondents, REMEDY
encouraged further participation in rheumatic and congenital
heart disease projects and collaboration with researchers in these
fields. At least eight sites have continued working with REMEDY
investigators on subsequent studies (INVICTUS, RHDGen
and Afrostrep) while independent sub-projects have focused
on pre-school screening for RHD, atrial fibrillation, primary
prevention measures for RHD, and co-morbid associations with
hepatitis B.
10
Administration: results varied when participants were asked
whether participation in REMEDY changed administrative
structures at their sites. Some (5/19) stated that it changed
systems for the filing of patient records and recording the
ECG machine
Echo machine
Stationery
Scanner
Airtime
Computer
Telephone
Other
1
6
6
10
13
11
5
6
0
2
4
6
8
10
12
14
Fig. 7.
Online survey: items purchased during REMEDY.
Penicillin
Anticoagulants
Other (e.g. digoxin)
Percentage of survey respondents
64
62
60
58
56
54
52
63.3
63.3
56.7
Fig. 6.
Online survey: drug stock-out problems.
90%
5%
5%
Impact
No answer
No impact
Fig. 8.
Telephone interview: impact of REMEDY on patient
management.